
Reducing outpatient drug-related problems through pharmacist- led interventions: A multi-center interventional study in provincial hospitals in Vietnam
Thang Nguyen*. PhD, Faculty of Pharmacy, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. nthang@ctump.edu.vn
Phuong Minh Nguyen. PhD, , Faculty of Medicine, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. nmphuong@ctump.edu.vn Tu Thi Cam Le. MSc, Faculty of Pharmacy, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. ltctu@ctump.edu.vn
Anh Nhut Lam. MSc, , Faculty of Public Health, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. lnanh@ctump.edu.vn
Hung Huynh Vinh Ly. MD, , Faculty of Medicine, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. lhvhung.ctump@gmail.com
Suol Thanh Pham. PhD, , Faculty of Pharmacy, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. ptsuol@ctump.edu.vn
Tan Thanh Nguyen. PhD, , Faculty of Medicine, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. nttan@ctump.edu.vn
Khanh Tuan Nguyen. PharmB, , Faculty of Pharmacy, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. ntkhanh.ds@gmail.com
Trang Thi Nhu Nguyen. MSc, , Office of Science and Technology – External Relations, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. ntntrang@ ctump.edu.vn
Tan Van Ngo. PhD, , Faculty of Public Health, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam. ngotansyt@gmail.com
Ngoc Thi Nhu Duong. MSc, , Department of Health, Vinh Long Province, Vietnam. ngocduongthinhu@gmail.com
Nghia Van Le. PhD, , Nguyen Dinh Chieu Hospital, Vinh Long Province, Vietnam. levannghia1972@gmail.com
DOI: 10.18549/PharmPract.2026.1.3487
Abstract
Background: Drug-related problems (DRPs) significantly affect patient safety, clinical outcomes, and healthcare efficiency. Pharmacist-led interventions have demonstrated potential in improving prescribing practices, yet limited data exist on their effectiveness in outpatient settings in Vietnam. This study evaluated the impact of structured pharmacist interventions on reducing DRPs in outpatient prescriptions at multiple healthcare facilities in a province in Vietnam. Methods: A pre-post interventional study was conducted at three hospitals in a province in Vietnam. Pharmacists systematically reviewed outpatient prescriptions identified DRPs using version v9.1 of the Pharmaceutical Care Network Europe (PCNE) classification and selected criteria from Vietnam’s Ministry of Health classification, and provided structured interventions, including quarterly seminars, hospital DRP bulletins, and personalized physician-specific DRP information sheets. Multivariate logistic regression assessed factors associated with DRP. Results: In total, 4,070 prescriptions preintervention and 4,051 prescriptions post-intervention were analyzed. Pharmacist-led interventions significantly reduced the proportion of prescriptions with at least one DRP from 21.7% (pre-intervention) to 9.1% (post-intervention; p<0.001). Significant reductions were observed across multiple DRP categories, including inappropriate drug indications, contraindicated medications, unnecessary drug prescriptions, incorrect dosing, improper timing of administration, and clinically significant drug-drug interactions (p<0.001). Factors independently associated with higher DRP risk included patient age ≥60 years (OR=1.554; p<0.001) and prescriptions containing five or more medications (OR=2.435; p<0.001). Proton pump inhibitors, gastrointestinal motility regulators, and non-steroidal anti-inflammatory drugs (NSAIDs) were most frequently implicated in DRPs. Conclusions: Pharmacist-led interventions effectively reduced DRPs in outpatient prescriptions at provincial hospitals in Vietnam. Older patients and those receiving polypharmacy were at higher risk, highlighting the need for targeted pharmaceutical care. This intervention model is practical, scalable, and well-suited for integration into electronic prescribing systems, significantly enhancing medication safety and prescribing quality.
Keywords: Drug-related problems, pharmacist intervention, outpatient prescribing, clinical pharmacy, Vietnam
INTRODUCTION
Drug-related problems (DRPs) continue to represent a significant global healthcare challenge, negatively impacting patient safety, clinical outcomes, and healthcare expenditures1,2,3. DRPs encompass multiple prescribing issues, including inappropriate medication selection, incorrect dosing, potential drug interactions, and deviations from established clinical guidelines4,5. These problems substantially compromise medication effectiveness and patient safety, underscoring the urgent need for structured interventions to enhance prescribing quality and medication management6,7. Recent international studies emphasize that DRPs remain prevalent across healthcare settings, particularly in outpatient care, highlighting significant gaps in current medication management practices globally8,9.
Internationally, DRPs persist at high levels across diverse patient populations. For instance, recent research in France indicated that 77.4% of patients had at least one identified DRP in their prescriptions10. Similarly, a study conducted in Indonesia revealed DRPs in approximately 57.0% of outpatient prescriptions, predominantly involving inappropriate medication use11. Such issues lead to reduced patient quality of life, increased morbidity, and elevated mortality rates, emphasizing the essential role pharmacists play in proactively identifying, preventing, and managing DRPs to optimize therapeutic outcomes12,13.
In Vietnam, DRPs are frequently reported in outpatient settings, commonly characterized by excessive antibiotic prescribing, incorrect dosage regimens, and inadequate prescribing documentation14,15,16. These issues arise from multiple factors, including increased healthcare demands, widespread polypharmacy, limited clinician access to current prescribing guidelines, and underdeveloped structured mechanisms for effective DRP management, particularly at the provincial outpatient level17,18,19.
Pharmacists have a pivotal role in addressing DRPs through comprehensive interventions spanning the medication-use continuum, from prescription review to patient counseling and education20,21. Robust international evidence consistently supports pharmacist-led interventions in significantly reducing DRP incidence, improving medication adherence, and enhancing clinical outcomes22,23,24. Recent global studies have further reinforced this evidence, demonstrating notable improvements in medication safety and patient outcomes across varied healthcare contexts, including community pharmacies and outpatient clinics25,26,27. However, evidence remains limited regarding pharmacist interventions specifically targeting outpatient prescribing practices in provincial hospitals in Vietnam.
This study addresses this critical knowledge gap by evaluating the impact of structured pharmacist-led interventions on prescribing quality in outpatient departments of provincial hospitals in Vietnam. The primary objectives are to systematically identify and classify common DRPs, implement targeted pharmacist interventions, and evaluate their effectiveness in reducing DRP prevalence and enhancing prescribing quality. The results of this study aim to strengthen clinical pharmacy practices and substantially contribute to medication safety initiatives both nationally and internationally.
METHODS
Study design
This was a pre-post multi-center interventional study designed to evaluate the impact of pharmacist-led interventions on outpatient prescribing practices by comparing outcomes before and after the intervention.
Study population and setting
The study included outpatient prescriptions collected from three hospitals in a province in Vietnam: one provincial general hospital and two district-level general hospitals. Prescriptions were collected in two phases: pre-intervention (April 1–June 30, 2020) and post-intervention (April 1–May 31, 2022).
Participating physicians comprised 27 from the provincial general hospital, 17 from one district hospital, and 21 from the other district hospital, all actively working in outpatient departments during the study periods.
Inclusion criteria
- Outpatient prescriptions from the hospitals’ outpatient departments.
- Adult patients aged ≥18 years.
- Physicians are actively involved in outpatient treatment during the study periods.
Exclusion criteria
-
Repeated prescriptions for the same patient with identical diagnoses within one month.
-
Prescriptions for pregnant patients.
-
Prescriptions from physicians are absent due to leave or training during data collection periods.
Study timeline
The study was conducted from June 2020 to May 2022, structured as follows:
-
Pre-intervention data collection: April 1–June 30, 2020 (all hospitals).
-
Main interventions: April 1–7, 2022 (provincial hospital), April 8–15, 2022 (first district hospital), April 16–24, 2022 (second district hospital).
-
Reinforcement interventions: Following the main interventions, from April 8–May 7, 2022 (provincial hospital), April 16–May 16, 2022 (first district hospital), and April 25–May 25, 2022 (second district hospital).
-
Post-intervention data collection: Conducted immediately after each hospital’s respective main intervention.
Sample size calculation
The sample size aimed to detect changes in the proportion of prescriptions containing at least one DRP. Using an expected DRP prevalence (p = 0.89 from previous research by Nguyen Anh Nhut8), a confidence interval of 95% (Z = 1.96), and an allowable error margin of 1%, the calculated minimum sample size per phase was approximately 3,761 prescriptions. Accounting for a potential 5% data loss, at least 4,000 prescriptions per study phase were targeted, resulting in a total of at least 8,000 prescriptions.
Sampling technique
Systematic random sampling was used to select prescriptions from each hospital during both pre- and post-intervention periods.
Study procedures
Pre-intervention phase
- Data collection: Patient demographic data (age, gender, insurance), diagnosis, clinic details, and comprehensive medication data (generic/brand names, dosage form, strength, frequency, timing relative to meals, total medications prescribed) were recorded.
- DRP identification: Clinical pharmacists identified DRPs by referencing standard resources, including drug manufacturer leaflets, the Vietnam National Drug Formulary, hospital-specific protocols, and guidelines issued by the Vietnamese Ministry of Health.
- Expert validation: Identified DRPs were reviewed by a nine-member expert panel. DRPs receiving consensus from ≥5/9 panelists were accepted; those without clear consensus underwent further discussion for resolution3.
DRP categories
DRPs were systematically classified according to Vietnam Ministry of Health guidelines (Decision No. 3547/QĐ-BYT) and Pharmaceutical Care Network Europe (PCNE) Classification v9.1, including1:
- Indication issues (e.g., unnecessary medication, contraindications).
- Dosage errors (excessive or inadequate daily doses).
- Frequency errors (excessively frequent or infrequent medication administration).
- Timing errors (incorrect administration relative to meals or daily schedule).
- Clinically significant drug interactions (identified via Drugs. com).
Intervention phase
Pharmacist-led interventions, developed based on preintervention findings, included5,6:
- Short educational seminars (10–15 minutes), highlighting identified DRPs and corrective actions.
- Informational flyers placed in physicians’ work areas summarizing key DRP cases and best practices.
- Direct pharmacist-to-physician discussions providing immediate feedback on prescribing issues.
Post-intervention phase
Post-intervention prescriptions underwent identical DRP analysis and categorization as in the pre-intervention phase. Outcomes evaluated included changes in the overall proportion of prescriptions containing DRPs and individual DRP types.
Statistical analysis
Data were analyzed using IBM SPSS Statistics v23.0. Descriptive statistics were used for continuous (mean) and categorical (% frequencies) variables. Chi-square tests compared DRP proportions before and after interventions. Independent t-tests and Mann-Whitney U tests assessed differences in continuous data across study phases. Logistic regression analyses identified factors influencing DRP occurrence. Statistical significance was set at p<0.05.
Ethical considerations
Ethical approval was obtained from the Ethics Committee of Can Tho University of Medicine and Pharmacy. Data confidentiality was ensured, with anonymized patient and physician information maintained throughout the study. Results were used solely for academic research purposes.
RESULTS
Characteristics of study samples
A total of 4,070 prescriptions were collected in the preintervention phase, and pharmacist interventions were subsequently conducted with prescribing physicians. Postintervention evaluation included 4,051 prescriptions. Characteristics of prescriptions before and after the intervention are summarized in Table 1.
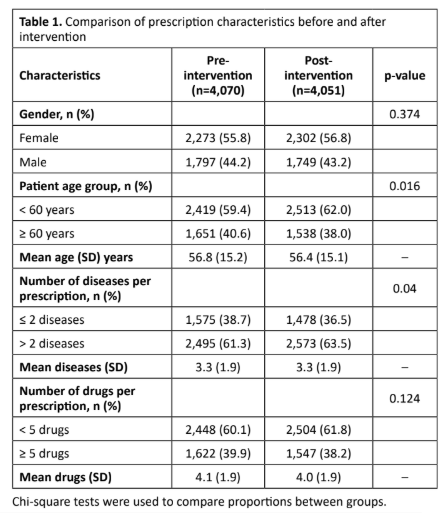
Significant differences were found in patient age groups (p = 0.016) and the number of diseases per prescription (p = 0.040). No significant differences were observed in gender distribution or the number of drugs per prescription.
Overall Effectiveness of Pharmacist Interventions on DRP
The effectiveness of pharmacist interventions on the overall incidence of drug-related problems (DRPs) is summarized in Table 2.
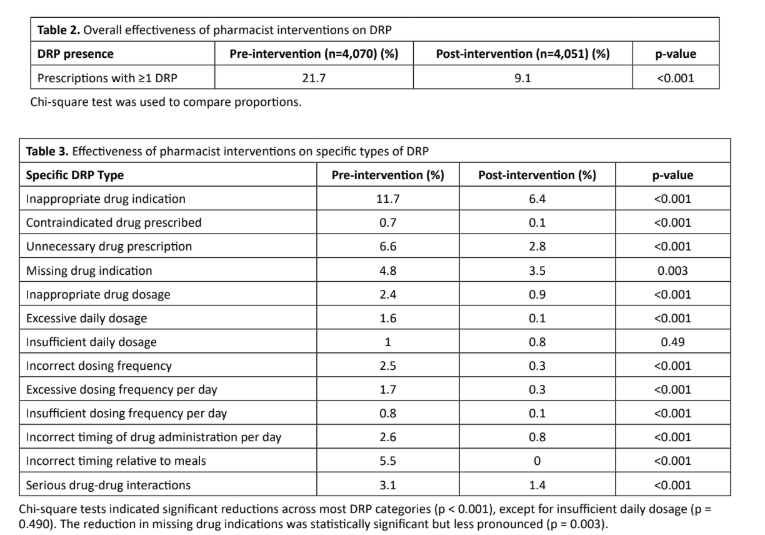
The proportion of prescriptions containing at least one DRP significantly decreased after pharmacist interventions (from 21.7% to 9.1%, p < 0.001).
Effectiveness of Pharmacist Interventions on Specific DRP Types
The effectiveness of pharmacist interventions on specific DRP categories is detailed in Table 3.
Overall, pharmacist-led interventions effectively improved prescribing practices, notably regarding appropriateness of drug indication, dosage accuracy, timing, and management of drug interactions.
Factors Associated with Drug-Related Problems (DRPs)
Multivariate logistic regression was conducted to identify independent predictors of DRPs. Results are presented in Table 4.
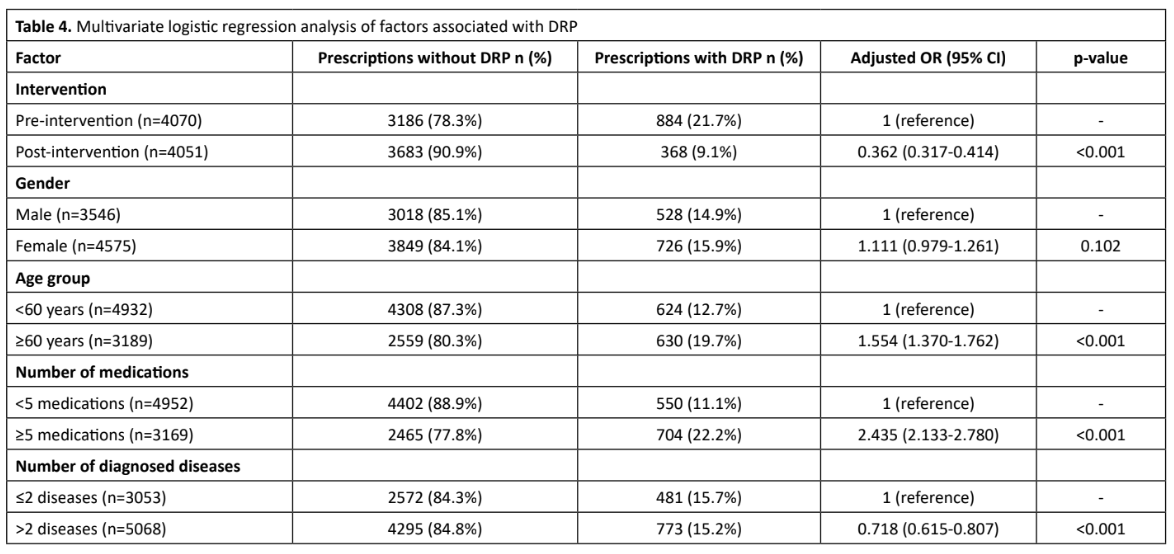
Patients aged ≥60 years (OR = 1.554; 95% CI: 1.370-1.762; p < 0.001) and prescriptions containing ≥5 medications (OR = 2.435; 95% CI: 2.133-2.780; p < 0.001) were significantly associated with an increased risk of DRPs. Prescriptions with more than two diagnosed diseases were associated with a reduced risk of DRPs (OR = 0.718; 95% CI: 0.615-0.807; p < 0.001). Gender was not significantly associated with DRP occurrence (p = 0.102).
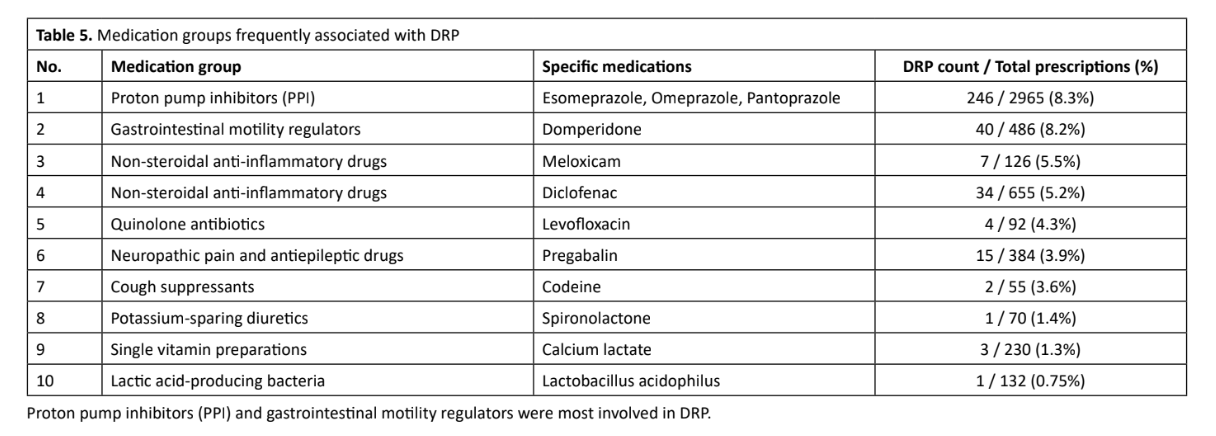
Medication Groups Frequently Associated with DRPs
Medication groups frequently involved in DRPs identified during the study period are listed in Table 5.
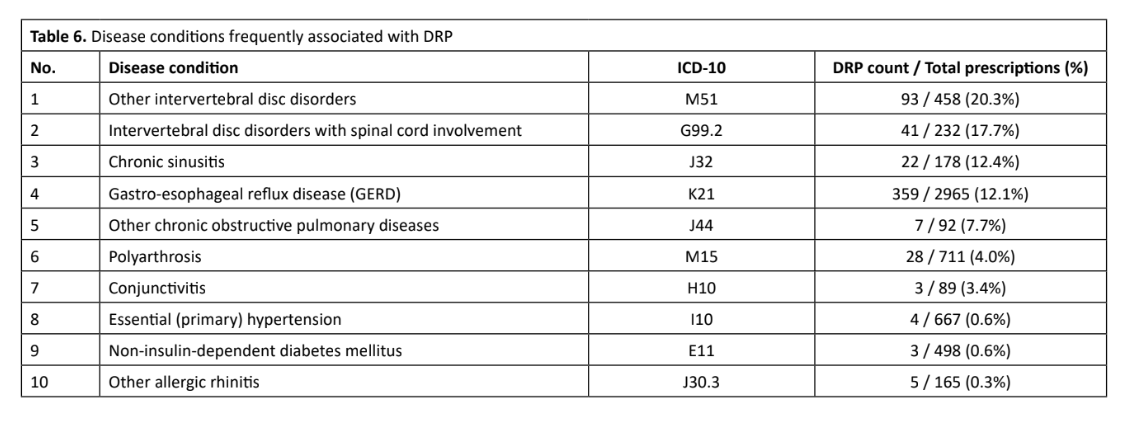
Disease Conditions Frequently Associated with Drps
Disease conditions commonly associated with DRPs in this study are summarized in Table 6.
Diseases most frequently associated with DRPs were intervertebral disc disorders, chronic sinusitis, and gastroesophageal reflux disease (GERD).
Intervertebral disc disorders, chronic sinusitis, and gastroesophageal reflux disease (GERD) were most associated with DRP.
DISCUSSION
This study demonstrated that structured pharmacist-led interventions significantly reduced drug-related problems (DRPs) in outpatient prescriptions at provincial hospitals in Vietnam. Specifically, the intervention decreased prescriptions containing at least one DRP from 21.7% pre-intervention to 9.1% post-intervention (p < 0.001). These findings align closely with recent global research, underscoring pharmacists’ critical role in improving medication safety, prescribing quality, and patient outcomes22,27.
Detailed analysis revealed substantial reductions across various DRP categories, including inappropriate drug indications, contraindicated medications, unnecessary prescriptions, incorrect dosing, inappropriate timing, and drug-drug interactions. These outcomes reflect international evidence that highlights pharmacist interventions as effective
strategies to address common prescribing errors, enhance medication adherence, and improve clinical outcomes10,11,25,27. However, the intervention demonstrated limited effectiveness in addressing insufficient daily dosing, suggesting the need for further targeted education and system-level enhancements to prescribing practices.
Significant predictors of DRP occurrence identified in this study included older patient age (≥60 years) and polypharmacy (≥5 medications). These factors align with previous research emphasizing elderly patients’ increased vulnerability due to pharmacokinetic alterations, complex medication regimens, and multiple comorbidities3,9,13. Conversely, prescriptions involving more than two diagnosed conditions were associated with a lower DRP risk, potentially reflecting heightened clinical vigilance and careful prescribing behaviors in more complex clinical scenarios.
Medication groups frequently associated with DRPs included proton pump inhibitors, gastrointestinal motility regulators, and non-steroidal anti-inflammatory drugs (NSAIDs). This finding aligns with international concerns about inappropriate prescribing practices and the overuse of these medication classes, further highlighting the importance of pharmacist oversight in rationalizing medication use8,10,12. Chronic conditions most commonly associated with DRPs, such as intervertebral disc disorders, chronic sinusitis, and gastroesophageal reflux disease (GERD), underscore the necessity for cautious medication prescribing in chronic disease management12,16,18.
From a practical standpoint, these findings offer significant implications, especially in the context of Vietnam’s ongoing administrative restructuring, which is consolidating administrative units from 63 provinces to approximately 34. This consolidation is anticipated to increase patient volume and workload pressures in provincial healthcare facilities, thereby elevating the risk of medication errors and DRPs. Implementing structured pharmacist-led interventions, as demonstrated in this study, can effectively address these challenges by providing standardized, scalable solutions to improve prescribing safety, medication efficacy, and patient outcomes amidst increased healthcare demands14,17,19.
Moreover, in line with Vietnam’s national digital transformation strategy outlined in Resolution No. 52-NQ/TW and Decision No. 749/QĐ-TTg, integrating pharmacist-generated DRP data into electronic prescribing platforms could substantially enhance the sustainability and effectiveness of clinical pharmacy
services. Clinical pharmacists’ systematic identification, classification, and validation of DRPs provide essential data for national electronic health databases. Integrating these validated datasets into electronic prescribing systems and clinical decision support tools could significantly enhance prescribing accuracy, patient safety, and quality improvement nationwide24,28. Leveraging national-level DRP data could facilitate proactive identification of high-risk medications, potential drug interactions, and prescribing errors, ultimately improving therapeutic outcomes through big data analytics and artificial intelligence applications.
Structured pharmacist-led interventions effectively reduce DRPs, significantly improving outpatient prescribing quality in provincial hospitals. Given Vietnam’s administrative restructuring and national digital transformation goals, these interventions represent a critical strategy for sustainably enhancing medication safety, clinical pharmacy practice, and healthcare quality across Vietnam’s evolving healthcare landscape. Future research should explore randomized controlled trials, long-term clinical outcomes, and comprehensive economic analyses to further validate and expand these findings nationally and internationally.
CONCLUSIONS
Pharmacist-led interventions significantly reduced drug-related problems (DRPs) in outpatient prescriptions, emphasizing pharmacists’ essential role in enhancing medication safety and prescribing quality. Older age (≥60 years) and polypharmacy (≥5 medications) were key predictors of DRP, highlighting the need for targeted interventions in these groups. The structured intervention model is practical and scalable nationwide, especially considering Vietnam’s administrative restructuring and digital transformation goals. Future research should extend the intervention to diverse healthcare settings, evaluate long-term outcomes, and integrate pharmacist-validated DRP data into electronic prescribing systems to support optimal medication management nationwide.
CONFLICTS OF INTEREST
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Pharmaceutical Care Network Europe Association. PCNE-Classification v9.1. 2020 [cited 2024 May 25]. Available from: https://www.pcne.org/upload/files/413_PCNE_classification_V9-1_final.pdf
- Al-Azzam S, Alzoubi K, Aburuz S, Alefan Q. Drug-related problems in a sample of outpatients with chronic diseases: a crosssectional study from Jordan. Ther Clin Risk Manag. 2016;12:233-239.
- Kaufmann CP, Stampfli D, Hersberger KE, Lampert ML. Determination of risk factors for drug-related problems: a multidisciplinary triangulation process. BMJ Open. 2015;5(3):e006376.
- Qassemi S, Pagès A, Rouch L, Bismuth S, Stillmunkes A, Lapeyre-Mestre M, McCambridge C, Cool C, Cestac P. Potentially inappropriate drug prescribing in French nursing home residents: an observational study. Pharmacy. 2020;8(3):133.
- Nguyen KT, Le VTT, Nguyen TH, Pham ST, Nguyen PM, Taxis K, Vi MT, Nguyen T, Tran HD. Effect of Pharmacist-Led Interventions on Physicians’ Prescribing for Pediatric Outpatients. Healthcare. 2022; 10(4):751.
- Sagita VA, Bahtiar A, Andrajati R. Evaluation of a clinical pharmacist intervention on clinical and drug-related problems among coronary heart disease inpatients: a pre-experimental prospective study at a general hospital in Indonesia. Sultan Qaboos Univ Med J. 2018;18(1):e82-e87.
- Vietnam Ministry of Health. Decision No. 4041/QĐ-BYT on the approval of the proposal to strengthen the control of prescription and prescription drug sales for the period 2017–2020. Hanoi: Ministry of Health; 2017.
- Nguyen NA, Nguyen T, Pham ST, Nguyen TH. Pharmacist-led interventions to reduce drug-related problems in prescribing for Vietnamese outpatients. Pharm Sci Asia. 2022;49(1):106–113.
- Nguyen HT, Bero L. A systematic review of drug-related problems in Vietnam: prevalence, causes and interventions. J Clin Pharm Ther. 2021;46(4):918-928.
- Vo TH, Bedouch P, Nguyen TH, et al. Pharmacy practice in Vietnam: current situation, challenges, and future perspectives. Res Social Adm Pharm. 2020;16(10):1352-1358.
- Allen B, Williams M, Peterson GM. Pharmacist-led medication reviews to identify and collaboratively resolve drug-related problems in psychiatry – a controlled clinical trial. PLoS ONE. 2016;10(11):e0142011.
- Frankenthal D, Lerman Y, Kalendaryev E, Lerman Y. Intervention with the screening tool of older persons potentially inappropriate prescriptions/screening tool to alert doctors to right treatment criteria in elderly residents of a chronic geriatric facility: a randomized clinical trial. J Am Geriatr Soc. 2014;62(9):1658-1665.
- Mekonnen AB, McLachlan AJ, Brien JE. Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: a systematic review and meta-analysis. BMJ Open. 2016;6(2):e010003.
- Liao Y, Ma C, Zhu H, et al. Impact of pharmacist intervention on the prescription of potentially inappropriate medication in elderly patients: a systematic review and meta-analysis. Eur J Clin Pharmacol. 2021;77(2):271-282.
- Ayhan YE, Aksoy M, Abdulrahman Y, Şahin Eröksüz ZS, Vezir D, Mercümek B, Bektay MY, Karakurt S, Sancar M. Evaluation of the effect of management of drug-related problems on clinical outcomes of pulmonary embolism outpatients: A randomized controlled trial. J Clin Med. 2025;14(4):1202.
- Tantipinichwong N, Keller MS. Operation Polypharmacy: a pharmacist-led ambulatory care clinic design and evaluation for older patients. Sci Rep. 2024;14:31719.
- Al-Taani GM, Muflih SM, Al-Azzam SI, Alzoubi KH. Costs saved and avoided from pharmacist interventions to address drugrelated problems identified in outpatient clinics in Jordan. PLoS One. 2024;19(6):e0302287.
- Riley K, Yap K, Foley G, Lambe J, Lund S. Impact of a clinical decision support system on identifying drug-related problems and making recommendations to providers during community pharmacist-led medication reviews in Ontario, Canada: A pilot study. J Eval Clin Pract. 2025;31(2):e14123.
- Ensing HT, Kurt N, Janssen RA, Koster ES, Heerdink ER. Pharmacist-led New Medicine Service: a real-world cohort study in the Netherlands on drug-related problems, satisfaction, and self-efficacy in cardiovascular patients transitioning to primary care. Int J Clin Pharm. 2025;47:325-334.
- Albabtain B, Bawazeer G, Paudyal V, Cheema E, Alqahtani A, Bahatheq A, Price MJ, Hadi MA. Impact of a community pharmacybased medication therapy management program on clinical and humanistic outcomes in patients with uncontrolled diabetes: A randomised controlled trial. Sci Rep. 2024;14:17818.
- Fentie AM, Huluka SA, Gebremariam GT, Gebretekle GB, Abebe E, Fenta TG. Impact of pharmacist-led interventions on medication-related problems among patients treated for cancer: A systematic review and meta-analysis of randomized control trials. Res Social Adm Pharm. 2024;20(5):487-497.
- Qassemi S, Rouch L, Bismuth S, Stillmunkes A, Lapeyre-Mestre M, McCambridge C, Cestac P. Potentially inappropriate drug prescribing in French nursing home residents: an observational study. Pharmacy (Basel). 2020;8(3):133.
- Kusumawardani LA, Andrajati R, Nusaibah A. Drug-related problems in hypertensive patients: A cross-sectional study from Indonesia. J Res Pharm Pract. 2020;9(3):140.
- Vietnam Ministry of Health. Decision No. 749/QĐ-TTg. National Digital Transformation Program until 2025, orientation towards 2030. Hanoi: Ministry of Health; 2020.
- Communist Party of Vietnam. Resolution No. 52-NQ/TW. Guidelines and Policies for Active Participation in the Fourth Industrial Revolution. Hanoi: Central Committee of the Communist Party; 2019.
- Prime Minister of Vietnam. Decision No. 376/QĐ-BYT. Implementation plan for digital transformation in the health sector until 2025. Hanoi: Government Office; 2021.
- Hoang HT, Nguyen BT, Dang TT, et al. Leveraging digital health for clinical pharmacy development in Vietnam: current status and future directions. Pharm Pract. 2022;20(4):2774.
- Le VH, Tran TTH, Pham TP, et al. Digital transformation in Vietnamese healthcare: opportunities and challenges for clinical pharmacy services integration. Digit Health. 2023;9:20552076231168034.