
Assessing knowledge of village health volunteers on pharmaceutical consumer protection and unsafe health products in Thailand
Ruethairat Srikwan. Pharmacist, Ko Chan Hospital, Chonburi Provincial Public Health Office, Chonburi, Thailand. ruethairatsrikwan@gmail.com
Ganrawee Khlaewkhlad. Public Health Technical Officer, Ko Chan District Public Health Office, Chonburi Provincial Public Health Office, Chonburi, Thailand.
Prayuth Poowaruttanawiwit*. Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Naresuan University, Phitsanulok, Thailand. Yuth_pu@hotmail.com
DOI: 10.18549/PharmPract.2026.1.3536
Abstract
Background: Village health volunteers (VHVs) are pivotal to Thailand’s primary care and increasingly engage in pharmaceutical consumer protection; however, evidence linking their knowledge to role perception and personal factors is limited. Objective: To measure VHVs’ knowledge of health consumer protection, examine associations with personal and role-related factors, and inform targeted training and policy. Methods: Cross-sectional census of active VHVs in Ko Chan District, Chonburi (n=270). A validated questionnaire captured demographics, role perception, and a 10-item knowledge test (0–10; also categorized). Descriptive statistics, group comparisons, Pearson/Spearman correlations, and multivariable logistic regression (outcome: high knowledge ≥80%) were applied (α=0.05). Results: Mean knowledge was 6.71±0.92 (median 7, IQR 6–7); mean role perception was 37.13±4.92 (median 36, IQR 34–41). Correlations between role perception and knowledge were non-significant (Pearson r=0.027, p=0.664; Spearman ρ=0.073, p=0.232). Logistic regression identified no independent predictors of high knowledge: role perception AOR 0.956 (95% CI 0.873–1.047; p=0.337); prior training AOR 0.691 (0.271–1.758; p=0.437); years of service and other demographics also non-significant, with some subgroup estimates imprecise due to sparsity. Conclusions: VHVs demonstrated moderate knowledge with limited variability and no detectable effects of role perception, training, or service duration. Findings support universal, competency-based refresher training and structured CPD aligned with pharmacy-practice priorities (e.g., recognition/reporting of substandard/falsified products) to strengthen community-level pharmaceutical safety.
Keywords: village health volunteers, consumer protection, role perception, knowledge assessment
INTRODUCTION
Village health volunteers (VHVs) are a cornerstone of Thailand’s primary healthcare system, serving as the critical interface between communities and formal health services. Established as part of the country’s primary healthcare–strengthening strategy, VHVs have long delivered health education, promoted disease prevention, facilitated early detection, and supported referrals to higher levels of care1,2. Their remit has increasingly expanded to health consumer protection, encompassing the identification, reporting, and prevention of unsafe services and substandard/falsified medical products across medicines, traditional remedies, dietary supplements, herbal products, and cosmetics—sectors that have proliferated and vary in quality, safety, and regulatory compliance3,4. Global and national surveillance consistently document the burden of Substandard and Falsified (SF) medical products: WHO reports substantial public-health and economic impacts, and the Thai FDA records regular enforcement actions against illegal or unsafe health products. Together, these patterns underscore the need for community-level pharmaceutical consumer protection and position VHVs as frontline contributors to pharmacovigilance and rational medicine use5,6.
The effectiveness of VHVs in safeguarding community health in this domain depends on two key factors: the adequacy of their knowledge and their clarity of role perception. Knowledge equips VHVs with the capacity to recognize product-related hazards and take appropriate action, while role perception— defined as the extent to which individuals understand, internalize, and value their professional responsibilities— shapes their motivation and commitment to fulfilling these duties5. International and national studies have underscored that targeted training programs can improve VHV competencies; however, evidence suggests that such improvements may not always be sustained over time, and the magnitude of training effects varies. While some studies report that years of service and higher educational attainment correlate with better knowledge retention, other findings suggest these factors may have limited or inconsistent influence6,7. The relationship between role perception and knowledge in the specific context of health consumer protection remains underexplored, particularly in Thailand. Previous research in other public health domains has shown that strong role perception can enhance performance, community trust, and engagement in preventive activities. However, without empirical evidence in consumer health protection, it is unclear whether role perception similarly contributes to knowledge acquisition or application in this field. Moreover, gaps in understanding these associations may hinder the development of effective training, support mechanisms, and policy measures aimed at strengthening VHVs’ capacity to carry out their consumer protection responsibilities8.
Motivated by these considerations, we focused on village health volunteers (VHVs) in Ko Chan District, Chonburi, to address a prespecified question: What is the level of healthconsumer protection knowledge among VHVs, and how is it associated with personal factors and role perception? Our priori hypothesis was that higher role-perception scores, prior training in health-consumer protection, and longer service duration would be independently associated with higher knowledge scores. To support internal validity, we defined knowledge as the primary outcome, treated personal factors and role perception as prespecified independent variables, and planned analyses before data inspection to minimize selective reporting; effect sizes with confidence intervals were to be estimated using multivariable models to mitigate plausible confounding.
To strengthen the pharmacy-practice orientation, we explicitly position VHVs within Thailand’s pharmaceutical consumer-protection system, where a substantial share of community complaints and hazards involves medicines, traditional remedies, dietary supplements, and cosmetics. In this framework, VHV knowledge is not generic “consumer protection” but a frontline determinant of pharmaceutical regulation and rational drug use: recognizing and reporting suspect or substandard/falsified products, supporting postmarketing surveillance and referral to regulatory authorities, reinforcing safe self-medication and adherence, and triggering timely pharmacist or facility review when adverse effects or inappropriate use are suspected.
Accordingly, if knowledge levels are only moderate, this implies targetable capacity gaps in medicine-related hazard identification, reporting pathways, and patient counselling—domains directly linked to pharmacovigilance and quality use of medicines in primary care. Embedding pharmacy-linked competencies (e.g., recognition of highrisk medicines/supplements, structured ADR and qualitydefect reporting, and referral algorithms co-developed with community pharmacists) into VHV training and CPD would align with national pharmaceutical governance goals and enhance community-level drug safety and rational medicine use. Within this surveillance ecosystem, VHVs function as complementary extensions of the pharmacy workforce: they screen at community level for suspect products and unsafe use, while community pharmacists provide verification, patient counselling, and formal reporting to regulatory channels— together forming a bidirectional screen–verify–report– feedback loop that strengthens pharmaceutical consumer protection.
Objective
To (1) measure VHVs’ knowledge of health consumer protection; (2) test how knowledge is associated with personal and role-related factors; and (3) generate evidence to guide targeted training, continuing professional development, and policy actions that strengthen VHVs’ consumer-protection functions in community health systems.
RESEARCH METHODOLOGY
Study Design and Setting
This study employed a cross-sectional analytical design to assess the level of health consumer protection knowledge among VHVs and to examine its association with personal characteristics and role perception. The study was conducted in Ko Chan District, Chonburi Province, Thailand, an administrative area comprising both rural and semi-urban communities. Data collection was carried out during [insert month/year], ensuring coverage of all subdistricts under the district jurisdiction.
Population and Sampling
The target population consisted of all active VHVs registered with the local public health authority in Ko Chan District at the time of the study. Inclusion criteria were: (1) currently serving as a VHV; (2) aged 18 years or older; and (3) willing to provide informed consent. VHVs who were on extended leave or unable to participate due to illness were excluded. A census approach was applied, aiming to include all eligible VHVs (n = 270) to maximize representativeness and avoid sampling bias.
Instrument Development and Validation
Data were collected using a structured, intervieweradministered questionnaire comprising three sections:
- Demographic and Personal Characteristics: Age, gender, education level, monthly income, years of service, and prior training in health consumer protection.
- Role Perception: Measured using a Likert-scale instrument adapted from validated role perception tools in community health research, translated into Thai and culturally adapted following forward–backward translation protocols. Content validity was assessed by a panel of three experts, comprising two specialists in pharmacy practice and one university faculty member with expertise in community pharmacy, resulting in a Content Validity Index (CVI) of ≥0.80 for all items.
- Knowledge on Health Consumer Protection: A 10-item multiple-choice test covering regulatory requirements, identification of unsafe products, and reporting procedures. Items were developed from Ministry of Public Health guidelines and previously validated consumer protection training materials. Reliability testing was performed in a pilot group of 30 VHVs from a neighboring district, resulting in a Kuder–Richardson Formula 20 (KR-coefficient of ≥ 0.70, indicating acceptable internal consistency.
Data Collection Procedures
Trained data collectors, all of whom were health professionals familiar with VHV activities, administered the questionnaire in face-to-face sessions at community health centers. Prior to data collection, the purpose and procedures of the study were explained, and written informed consent was obtained. To minimize interviewer bias, data collectors received standardized training on questionnaire administration, and the same instructions were read to all participants.
Variable Definitions
The primary outcome was a knowledge score derived from a 10-item multiple-choice instrument. Scores were analyzed both as a continuous total (0–10) and as an ordinal category (low, moderate, high) using pre-specified cut-offs. Explanatory variables included personal characteristics (age, sex, education, income, prior training, years of VHV service) and a role-perception score. To reflect the complementary VHV– pharmacist interface in community drug-safety surveillance, the role-perception scale explicitly incorporated pharmacistcollaboration tasks (e.g., signal recognition, referral to pharmacy services, and awareness of pharmacist-led reporting pathways). For interpretability and content validity, we adopted WHO definitions of substandard and falsified medical products and aligned item wording with Thai FDA regulatory categories (medicines, traditional remedies, dietary supplements, cosmetics)1,2.
Statistical Analysis
Descriptive statistics were used to summarize participant characteristics. Continuous variables were presented as mean ± standard deviation (SD) or median and range, depending on distribution; categorical variables were presented as frequency and percentage. Knowledge scores were compared across demographic subgroups using independent t-tests or ANOVA for normally distributed data, and Mann–Whitney U or Kruskal– Wallis tests for non-normally distributed data. Associations between role perception and knowledge score were examined using Pearson’s or Spearman’s correlation coefficients, as appropriate. Logistic regression analysis was conducted to identify independent predictors of high knowledge level (≥80% correct), with results reported as adjusted odds ratios (AOR) and 95% confidence intervals (CI). Statistical significance was set at p < 0.05. All analyses were performed using computer program.
Ethical Considerations
The study protocol was reviewed and approved by the Chonburi Provincial Health Office Institutional Review Board (approval number: CBO Rec 2568-013). All participants provided written informed consent prior to participation. Confidentiality was maintained by anonymizing data, and responses were stored securely with access limited to the research team.
RESULTS
The study included 270 village health volunteers (VHVs) from Ko Chan District, Chonburi Province. As shown in Table 1, the
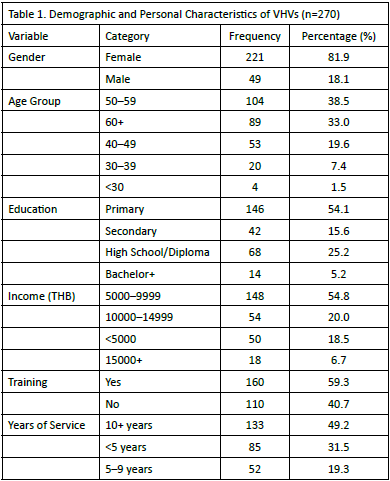
majority were female (81.9%) and aged between 50–59 years (38.5%), followed by those aged 60 years or above (33.0%). Most participants had a primary (54.1%) or high school/ diploma (25.2%) education, with smaller proportions holding a secondary (15.6%) or a bachelor’s degree or higher (5.2%). The majority (54.1%) reported a monthly income of 5,000–9,999 THB, while 20.0% each earned between 10,000–14,999 THB or less than 5,000 THB (18.5%), and 6.7% earned 15,000 THB or more. A majority had received prior training in health consumer protection (59.3%), and nearly half (49.2%) had served as VHVs for 10 or more years, 31.5% for less than 5 years, and 19.3% for 5–9 years.
As shown in Table 2, the role-perception score averaged 37.13 (SD 4.92; median 36; IQR 34–41), indicating a generally high selfreported understanding of assigned roles and responsibilities. The knowledge score averaged 6.71 (SD 0.92; median 7; IQR 6–7), reflecting a moderate-to-high level of health-consumerprotection knowledge. The narrow IQRs and small SDs for both measures suggest limited dispersion and a relatively homogeneous sample, providing a stable basis for comparative and correlational analyses. The 10-item instrument covered pharmacy-relevant domains—regulatory requirements, identification of unsafe products, and reporting procedures— across medicines, traditional remedies, dietary supplements, herbal products, and cosmetics. Within this framework, VHVs showed moderate overall knowledge with limited variability. Between-group tests found no significant differences by prior training or years of service, and multivariable models

identified no demographic or role-related predictors of high knowledge. Although items were not tagged by product class, the aggregate pattern indicates system-wide, pharmacy-facing gaps in hazard recognition and reporting, warranting universal, competency-based upskilling—specifically in (i) recognition of suspect or substandard/falsified products, (ii) safe selfmedication and adherence counselling, (iii) early identification of adverse effects and inappropriate use, and (iv) use of structured reporting/referral pathways (Thai FDA channels and pharmacist collaboration).
The distribution of knowledge scores among the 270 VHVs is presented in Figure 1. Most participants demonstrated a moderate level of knowledge (60–70%), followed by those in the high knowledge category (≥80%) and a smaller proportion in the low category (<60%) (Figure 1A). The mean knowledge score for the sample was 6.71, with a 95% confidence interval of 6.60 to 6.82, indicating a relatively narrow range and high precision in the estimate (Figure 1B). The error bar plot demonstrated that the mean knowledge score was positioned at the upper end of the moderate range, indicating generally adequate knowledge with scope for further improvement toward consistently high levels across the cohort. The small standard deviation and narrow confidence interval further support the internal consistency of the measure and reinforce the reliability of subsequent analyses.
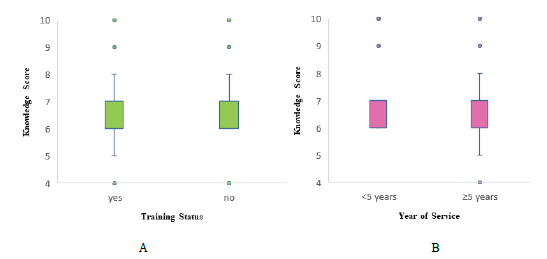
Figure 2 presents the comparative analysis of knowledge scores stratified by training status and years of service. VHVs who had received prior training in health consumer protection demonstrated a slightly higher mean knowledge score than those without training; however, the difference did not reach statistical significance (p = 0.792) (shown in figure 2A), indicating that training history alone may not be a sole determinant of knowledge level in this cohort. When stratified by years of service, no statistically significant difference was observed between VHVs with less than five years of service and those with five or more years (p = 0.063) (shown in figure 2B), suggesting that accumulated service duration does not independently predict higher knowledge scores in this sample. The narrow interquartile ranges in both comparisons indicate relatively homogeneous knowledge levels within each subgroup, further supported by the absence of extreme outliers. These findings highlight the need for targeted, ongoing educational interventions that address specific knowledge gaps rather than relying solely on accumulated service experience or past training participation to ensure uniformly high levels of health consumer protection knowledge among VHVs.
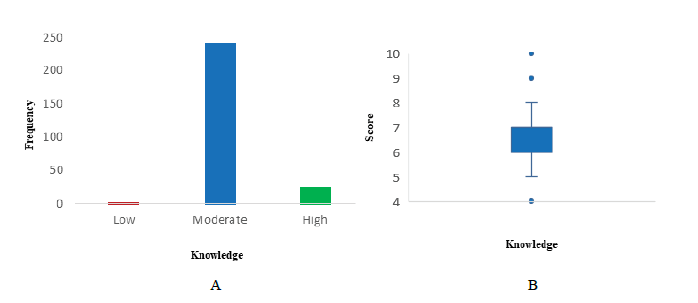
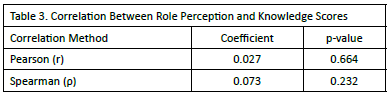
Table 3 summarizes the correlation analyses between role perception and knowledge scores among village health volunteers. Pearson’s correlation coefficient (r = 0.027, p = 0.664) and Spearman’s rank correlation coefficient (ρ = 0.073, p = 0.232) both indicated no statistically significant association between the two variables. These coefficients, which were both near zero, reflect a negligible level of association. The consistency of findings across both parametric (Pearson) and non-parametric (Spearman) approaches strengthens the conclusion that no meaningful relationship exists between role perception and knowledge scores in this study.
Table 4 presents the results of the multiple logistic regression analysis examining factors associated with achieving a high knowledge score (≥ 80%) among village health volunteers. After adjustment for potential confounders, none of the assessed variables demonstrated a statistically significant association with high knowledge levels. Role perception scores showed no measurable effect (AOR = 0.956; 95% CI: 0.873–1.047; p = 0.337). Volunteers with prior training had lower odds of attaining a high knowledge score compared with those without training, though this difference was not statistically significant (AOR = 0.691; 95% CI: 0.271–1.758; p = 0.437). Similarly,
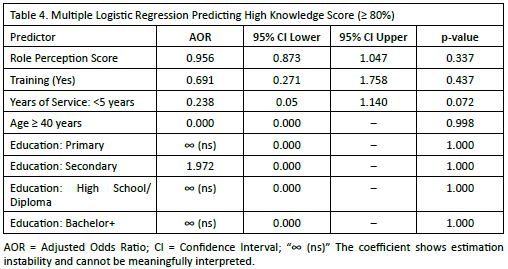
variations by years of service, age group, and education level did not reach statistical significance, with several subgroup estimates limited by sparse data. Overall, these findings indicate that high knowledge scores were not significantly influenced by the demographic or experiential characteristics measured in this cohort, underscoring the need to explore additional factors that may contribute to knowledge performance.
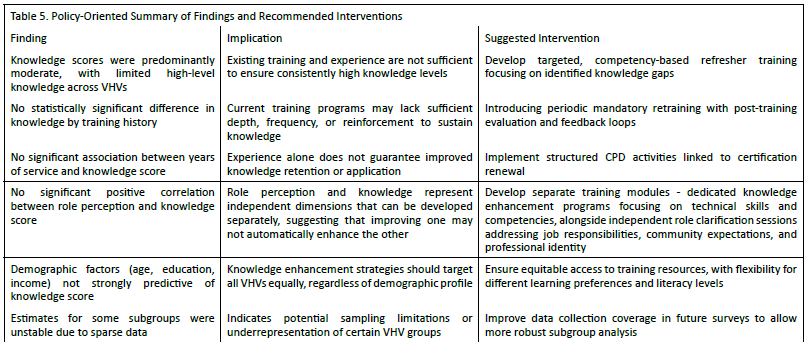
Table 5 links key findings to practical policy actions. Moderate knowledge levels among VHVs indicate the need for targeted, competency-based refresher training. The absence of significant differences by training history or years of service suggests current programs lack sufficient depth and reinforcement, supporting periodic retraining and structured CPD. The lack of correlation between role perception and knowledge scores the value of integrating role clarity modules into training.
Demographic factors were not strong predictors, indicating interventions should be universally accessible. Sparse subgroup data highlights the need for improved coverage in future studies.
DISCUSSION
This study assessed the level of health consumer protection knowledge among VHVs and examined its association with demographic characteristics, training history, years of service, and role perception. The findings indicate that most VHVs possessed moderate knowledge, with relatively few achieving high knowledge scores. The narrow range and small standard deviation of scores suggest limited variability within the cohort, indicating homogeneity in both knowledge and role perception.
This uniformity may reflect consistent baseline training and role expectations across the district but also points to limited differentiation in performance despite variation in service experience or prior training. Contrary to the initial hypothesis, neither prior training nor years of service showed a statistically significant association with higher knowledge scores. These results align with evidence from other community health worker studies indicating that experiential factors alone are insufficient to ensure sustained knowledge retention. Training history’s lack of measurable effect may be attributable to infrequent or non-standardized training content, absence of post-training evaluation, or insufficient reinforcement mechanisms. These findings are consistent with those reported by Charoenpong (2023), who observed that community health volunteers (CHVs) receiving only a single, non-continuous training session demonstrated knowledge that was not aligned with current health issues, potentially limiting their ability to deliver up-to-date health information9. In line with the World Health Organization (2018) guideline, Health Policy and System Support to Optimize Community Health Worker Programs, a comprehensive overview of 16 systematic reviews and additional review articles emphasized that CHVs should possess an appropriate minimum level of education, receive competency-based foundational training, and obtain formal certification. Furthermore, training should be systematically adapted to the community context, encompassing essential health knowledge, communication skills, and consumer protection principles. Both pre-service and ongoing inservice training were recommended to enhance work-related competencies and sustain performance over time10.
This study found no significant association between role perception and knowledge levels among VHVs. Although both Pearson’s and Spearman’s correlation coefficients demonstrated a weak positive relationship in the anticipated direction, the negligible magnitude and absence of statistical significance suggest that role perception did not meaningfully influence knowledge performance within this cohort. The consistency of the null finding across both parametric and nonparametric analyses enhances the robustness of this result.
These findings contrast with previous research highlighting the importance of role perception in CHV performance. Nunes and Lotta (2023) emphasized that educational attainment, work experience, social status within the community, and understanding of the health system shape role perception and subsequently improve CHVs’ effectiveness in service delivery and their relationships with community members11. Similarly, Mlotshwa et al. (2015) reported that CHVs frequently view themselves as a “bridge” between communities and the formal health system, enabling health knowledge dissemination and improving access to care. In these contexts, role perception functioned as a determinant of knowledge use and community engagement12.
The divergence of the current study’s results may be attributable to several factors. First, differences in measurement approaches may explain the discrepancy, as prior studies often assessed role perception qualitatively or within broader frameworks of community engagement. Second, unmeasured confounders such as motivation, organizational support, or variations in training quality may have influenced knowledge outcomes more strongly than role perception. Finally, contextspecific factors, including local health policies and community structures, may shape VHVs’ experiences differently from CHVs in other settings.
Overall, these results suggest that role perception alone is unlikely to serve as a reliable predictor of knowledge acquisition among VHVs. Future research should explore alternative pathways, including systemic support, ongoing training, and community engagement mechanisms, to better understand the determinants of knowledge performance in this workforce. In multivariable logistic regression, no demographic or rolerelated variables were independently associated with higher knowledge scores after adjustment for prespecified confounders. Because several subgroups had sparse observations, some estimates were imprecise and model stability was limited; thus, these null findings should be interpreted cautiously— they may reflect limited statistical power rather than a true absence of association. To strengthen internal validity in future studies, we recommend broader sampling with more balanced representation, an a priori sample-size/power calculation tailored to multivariable modeling, and—where small cells are unavoidable—use of penalized (e.g., Firth) or exact logistic methods to mitigate instability and residual confounding.
From a policy and implementation standpoint, the absence of strong demographic predictors supports universal, competency-based refresher training for VHVs, coupled with structured CPD that explicitly enhances role perception. Positioning VHVs to detect and report SF medical products is consistent with WHO surveillance guidance and complements Thai FDA post-marketing control; embedding signal recognition, reporting channels, and referral algorithms into CPD can tighten the local pharmacovigilance loop and promote rational medicine use1,2. Clarifying VHV–pharmacist complementarity further operationalizes community drug-safety surveillance: VHVs provide community-level screening and early signaling (e.g., suspected SF products, inappropriate self-medication), while pharmacists confirm, counsel, and complete formal ADR/quality-defect reporting to Thai FDA channels. Joint workflows—covering signal criteria, referral triggers, and feedback—should be incorporated into CPD to institutionalize this bidirectional “screen–verify–report–feedback” system.
In relation to the pharmacy-practice literature, community pharmacists are widely recognized as frontline actors in consumer protection and counterfeit/substandard medicine detection—verifying product quality, counselling on safe use, and completing ADR/quality-defect reporting to regulatory channels. Our findings, which show moderate VHV knowledge with no strong demographic or role-related predictors, reinforce a complementary model in which VHVs provide communitylevel screening and early signaling (e.g., suspected SF products or inappropriate self-medication), while pharmacists confirm, counsel, and formally report to Thai FDA pathways. Embedding this screen–verify–report–feedback workflow into joint VHV– pharmacist CPD (signal criteria, referral triggers, reporting channels) aligns the VHV role with established pharmacist functions in medicine-related consumer protection and helps close the last-mile gap in community pharmacovigilance.
CONCLUSION
Among VHVs in Ko Chan District, health-consumer-protection knowledge was moderate with limited variability, and no independent associations were detected with role perception, prior training, or years of service after adjustment. Given sparse subgroup data and the cross-sectional design, these null findings should be interpreted cautiously as they may reflect limited power rather than true absence of effect. Programmatically, results support universal, competency-based refresher training and structured CPD aligned with pharmacy-practice priorities (e.g., recognition and reporting of substandard/falsified products). Future studies should use larger, more balanced samples, pre-specified sample-size/power for multivariable analyses, item-level tagging by pharmaceutical domain, and (where small cells persist) penalized/exact logistic methods, ideally with pre–post and retention assessments to strengthen causal inference.
AUTHORS’ CONTRIBUTIONS
Ruethairat Srikwan (first author) led conceptualization, methodology, and project administration; coordinated site permissions and field operations; supervised data collection; performed formal analysis and data curation; and drafted the original manuscript. Ganrawee Khlaewkhlad (co-author) supported investigation and community engagement, contributed to instrument adaptation, data curation, and interpretation of findings, and provided writing—review & editing. Prayuth Poowaruttanawiwit (corresponding author) provided senior oversight on study design, pharmacypractice framing, and statistical methodology; ensured ethical compliance and internal-validity checks; led critical revision of the manuscript; and takes overall guarantor responsibility for the work. All authors read and approved the final version of the manuscript.
ACKNOWLEDGEMENT
Medical and Pharmacy Innovation Research and Development Unit, Faculty of Pharmaceutical Sciences, Naresuan University, Phitsanulok, Thailand
CONFLICT OF INTEREST
None to declared.
References
- World Health Organization. (1981). Global Strategy for Health for All by the Year 2000. World Health Organization.
- Bureau of Policy and Strategy, Ministry of Public Health. (2016). Thailand’s 20-year national strategic plan for public health sector. Retrieved November 27, 2024, from https://waa.inter.nstda.or.th/stks/pub/2017/201711117-MinistryofPublicHealth.
- Chuengsatiansup, K., & Suksut, P. (2007). Health volunteers in the context of change: Potential and developmental strategies. Health Systems Research Journal, 1(3–4), 268–279.
- Intharakhamhaeng, N. R. S., Rasiri, S., & Rasiri, T. (2021). The role of Thai public health volunteers. Journal of Health Systems Research, 14(3), 443–454.
- Yaebkai, Y., & Wongsawat, P. (2022). Factors affecting performance of village health volunteers in Sukhothai, Thailand. Journal of Public Health and Development, 20(1), 120–131.
- Abdel-All, M., et al. (2017). Effectiveness of community health worker training programmes for cardiovascular disease management in low-income and middle-income countries: A systematic review. BMJ Open, 7(e015529).
- Sultan, M. A., Miller, E., Tikkanen, R. S., Singh, S., Kullu, A., Cometto, G., Fitzpatrick, S., Ajuebor, O., Gillon, N., Edward, A., Moleman, Y. P., Pandya, S., Park, I., Shen, J. Y., Yu, Y., Perry, H., Scott, K., & Closser, S. (2025). Competency-based education and training for Community Health Workers: a scoping review. BMC Health Services Research, 25(1), 263.
- Kok, M. C., Dieleman, M., Taegtmeyer, M., Broerse, J. E., Kane, S. S., Ormel, H., Tijm, M. M., & de Koning, K. A. (2015). Which intervention design factors influence performance of community health workers in low- and middle-income countries? A systematic review. Health Policy and Planning, 30(9), 1207-1227.
- Charoenphong, S. (2023). Knowledge and health behaviors regarding consumer protection among village health volunteers in Lamphun Province. Journal of Health Consumer Protection, 3(1), 110-124.
- World Health Organization. (2018). WHO guideline on health policy and system support to optimize community health worker programmes. World Health Organization. https://www.who.int/publications/i/item/9789241550369
- Nunes, J., & Lotta, G. (2023). Are community health programmes always benign? Community health worker perceptions and the social construction of users in Brazil’s primary healthcare policy. Global Public Health, 18(1), 1-14.
- Mlotshwa, L., Harris, B., Schneider, H., & Moshabela, M. (2015). Exploring the perceptions and experiences of community health workers using role identity theory. Global Health Action, 8, 1-9.