
Attitude and needs of the community pharmacists in Abu-Dhabi Emirate in the United Arab Emirates about administering flu and COVID-19 vaccines: A cross-sectional study
Azhar T. Rahma*. Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates. Azhar.talal@uaeu. ac.ae
Ahmed Jihad. Burjeel Hospital, Al Ain, United Arab Emirates
Mohamud Sheek-Hussein. Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
Aminu S. Abdullahi. Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
Amer Mohammed Salem Alalawi. Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
Hamad Talal Jumaa Almaskari. Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
Mohamed Ahmed Ali Almarzooqi. Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
Omar Mohammed Salem Alalawi. Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
Sultan Majed Ibrahim Alhosani. Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
DOI: 10.18549/PharmPract.2025.3.3184
Abstract
Introduction: A rising number of countries have been enlarging the role of pharmacists to offer vaccination services, which magnified vaccination access and rates. The Department of Health in Abu Dhabi implemented changing the paradigm of community pharmacists’ role in Abu Dhabi to include administering both flu and COVID-19 vaccines to the public. Aims & Objectives: This study aims to explore and assess the needs and attitudes of the community pharmacists in Abu Dhabi about administering flu and COVID-19 vaccines and to explore their perceived challenges and enablers. Materials & Methods: A cross-sectional study design was adopted using a validated questionnaire. Ethical approval was obtained from the Social Research Ethics Committee, UAE University. Simple and multiple binary logistic regression models were used to identify factors associated with the willingness of the respondents to provide vaccine services. IBM SPSS was used for the data analysis. Results: The majority of the respondents were female (58.8%), married (58.9%), non- Emiratis (90.4%), and had more than five years of work experience (53.8%), in which at least one year working in the UAE (80.2%). The majority agreed that pharmacy students must be trained to administer vaccines and it should be part of the curriculum (81.0%). On the other hand, 82.2% of participants doubt the ability of their pharmacies to arrange a space for the administration of the vaccines. Having experience in administering subcutaneous (AOR=4.12, 95% CI=1.06-16.81, P=0.045), and having the belief that students should be trained (AOR=18.88, 95% CI=9.00-39.58, P<0.001) were significantly associated with willingness to administer vaccines after adjusting for confounders. Conclusion: The explored perspectives and needs of the community pharmacists will help stakeholders to have an evidence-based approach and strategy. Addressing the enablers and challenges will streamline the implementation of such initiatives in the seven Emirates of the UAE.
Keywords: Community pharmacists, COVID vaccine, Flu vaccine, Abu Dhabi
INTRODUCTION
A rising number of countries have been enlarging the role of pharmacists to offer vaccination services, which magnified vaccination access and rates1. The American Association of Hospital Pharmacists (ASHP) has endorsed guidelines on the pharmacist’s role in immunization, in their guidelines they stratified three spheres for the implementation of vaccine administration: legal, training, and program structure2. However, considering the novelty of this initiative in the United Arab Emirates (UAE), pharmacists’ perspectives and needs have to be factored in and taken into consideration. The majority of patients initially seek care from community pharmacists as they are identified as affordable and trusted providers with more flexible operating schedules1.As per Tawfiq et al 2021, “There are 143 hospitals in the UAE (45 governmental and 98 private), 7930 pharmacists (1814 in the governmental sector and 6116 in the private)”3. Pharmacists in the UAE must have a valid license to practice, whether they are clinical pharmacists, pharmacists, or pharmacy technicians.
Four pillars of vaccine administration by pharmacists had to be addressed, namely: legal authority, training, structure, and need. In the UAE, there are three regulatory bodies depending on the geographical location of the Emirates that pharmacists will practice. Namely, the Department of Health (Abu Dhabi region), Dubai Health Authority (Dubai region), and Ministry of Health and Prevention (Sharjah, Ajman, Umm Al-Quwain, Fujairah, and Ras Al Khaimah)4. Therefore, all of them had to legalize the administration of vaccines by pharmacists, or there would be fragmentation in the service. Additionally, in the UAE, there are different types of pharmacy licenses: Private pharmacy, hospital pharmacy, medical store, pharmaceutical factory, scientific office, pharmacist, and assistant pharmacist4. Therefore, the decision to add this role as the scope of service to pharmacists had to be tailored according to those different types of licenses. Furthermore, guidelines had to address the role of each type of pharmacy license as either/ or: (a) source of immunization information, (b) host of immunization sites, and (c) immunizers2.
The policy and practice guidelines have to enlist the needed competencies as well as their frequency (for example: Basic life support certification (BLS), advanced cardiac life support (ACLS) to handle reactions and anaphylactic shocks, annual competency, and hands-on vaccine administration competency). Additionally, there should be a key performance indicator (KPI) that is a measurable value that demonstrates how effective the objective of vaccine administration by pharmacists is2. Moreover, pharmacovigilance had to be vigilant to any trigger of administration errors in terms of route, frequency, site, and storage to evaluate this objective and be proactive, not reactive. A systematic review of the role of pharmacists in vaccination services in low and middle-income countries conducted in 2021 by Yemeke et al, concluded that better documentation of pharmacists’ contribution to vaccination services is vital to exhibit the significance of successful integration of pharmacists in immunization programs1.
Since most of the registered pharmacists in the UAE are expatriates and have obtained their undergraduate degrees from universities and colleges outside the country3. An attempt to explore the curriculum of a Bachelor of Pharmacy degree, and PharmD in Egypt, India, Pakistan, and Jordan (in which most of the expatriate pharmacists in the UAE are from) revealed that vaccine administration training was not offered to the students5-7. Additionally, mapping the curriculum of pharmacy degrees in the UAE mirrored the same findings8. Therefore, comprehensive training for pharmacists and technicians had to take place.
To sustain competency, pharmacists must gain access to recent immunization references (e.g., CDC’s National Immunization Program publications, including the “Pink Book”) and continuing education programs to stay well-informed of changing guidelines and recommendations2. A vaccine administration program requires a robust infrastructure of competent staff, physical space, and Policies and Procedures Guidelines (PPG) to guarantee the right vaccine storage and maintain the cold chain from the phase of receiving the vaccine till administering
it to the patients, as well as handling, patient screening and education, documentation, and billing and reimbursement1,2. Hence, for the Department of Health’s initiative to involve community pharmacists in the Emirate of Abu Dhabi to be successful, the roles of pharmacists, their perspectives, and needs have to be explored and tailored into the implementation strategy and procedures.
A study conducted in 2021 by Turcu-Stiolica A. et al about pharmacist’s perspectives on administering a COVID-19 Vaccine in community pharmacies in four Balkan countries concluded that the dearth of training in the faculty classes and the lack of a special place where to administer vaccines are associated with their hesitancy9. Supplementary factors were found in Bulgaria (pharmacists from independent pharmacies wanted more than the pharmacists working in chain pharmacies to administer vaccines) and in Serbia (male pharmacists agreed more with administering vaccines than female pharmacists)9.
For the Department of Health’s initiative to involve community pharmacists in the Emirate of Abu Dhabi to be successful, the roles of pharmacists, their perspectives, and needs have to be explored and tailored into the implementation strategy and procedures. Therefore, studies are needed to explore the needs of pharmacists in the United Arab Emirates as well as their perspectives and cultural aspects. Hence, this study aims to explore and assess the needs, and attitudes of the community pharmacists in Abu Dhabi Emirates about administering the Flu and COVID vaccines. Furthermore, we aim to explore the challenges and enablers that will streamline this initiative.
METHODOLOGY
To answer our research question, a cross-sectional study design had been adopted. A validated questionnaire used by Turcu-Stiolica A. et al (9) was used to screen the attitude of the community pharmacists in Abu Dhabi Emirate about administering flu and COVID-19 vaccine. The questionnaire is divided into three sections, demographics, attitude questions, and challenges and enablers. The questionnaire was translated into Urdu and we used back-to-back translation for validation.
The inclusion criteria were: Currently licensed as a community pharmacist or a trainee in Abu Dhabi Emirates, any nationality, understanding English or Urdu language, aged 18 years or older, and had consented to participate in the study. We obtained the sampling frame of all the community pharmacies in the Emirates of Abu-Dhabi, in the United Arab Emirates. Cluster sampling was employed by selecting community pharmacies from the main geographical areas in Abu Dhabi Emirates (Al Ain, Eastern region, Mussafah, Abu Dhabi city, industrial region, Wagan and Mazyed). We utilized both online platforms as well as visiting the community pharmacy located in Abu Dhabi Emirate with iPad or hardcopy questionnaires. The community pharmacies were visited onsite.
The purpose of this study had been explained, and they were asked to sign the consent form before taking the survey. The study was approved by the Social Research Ethics Committee of the United Arab Emirates University ERS_2022_8496.
To determine the sample size, the following formula was used where: n = sample size required, Z = the statistic corresponding to the 95% confidence level = 1.96, p = estimated prevalence = 0.39, q = 1-p = 0.71, d = maximum allowable error in the estimate of the prevalence = 0.05. The final calculated sample size was 428.
The survey respondents were summarized based on socio-demographic characteristics using frequencies and percentages. Similarly, survey responses based on the specific items were presented as frequencies and percentages. Binary logistic regression was used to identify factors associated with the willingness of the respondents to provide vaccine services. In the model, willingness was used as the outcome variable while other variables including socio-demographics and other relevant variables were employed as independent variables. Univariate binary logistic regression was first performed to explore the association between willingness and several factors. For the final adjusted model, multiple binary logistic regression analysis was performed including only those factors found to be significantly associated with the outcome variable in the univariate analysis. A P value of < 0.05 was considered statistically significant. IBM SPSS Statistics for Windows, Version 28.0 was used for the analysis.
RESULTS
Participants’ characteristics
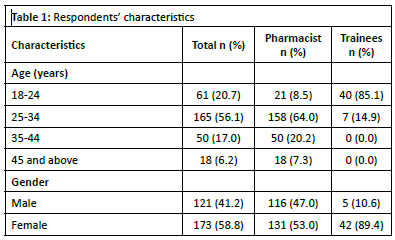
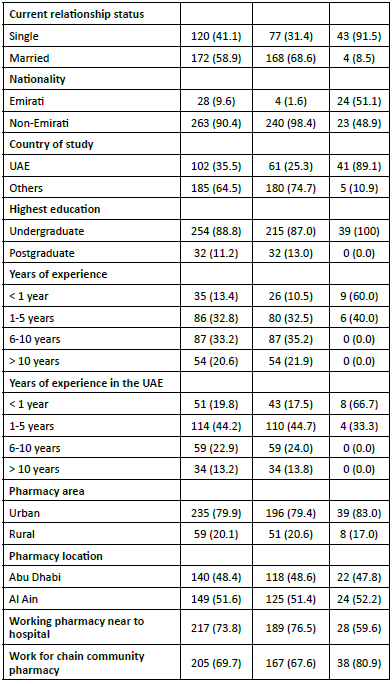
The characteristics of the participants and their pharmacy place of work are presented in Table 1. More than half (56.1%) of the participants were between the ages of 25 to 34 years as those 45 and above years constituted the minority in the sample (6.2%). The majority of the respondents were female (58.8%), married (58.9%), non-Emiratis (90.4%), and had at most an undergraduate qualification (88.8%), had more than five years of work experience (53.8%), and had spent at least one year working in the UAE (80.2%). Regarding the pharmacy place of work, the majority of the respondents worked in a pharmacy located in an urban area (79.9%), in the city of Al Ain (51.6%), near a hospital or clinic (73.8%), as well as being a chain community pharmacy (69.7%).
Attitude toward administering vaccines
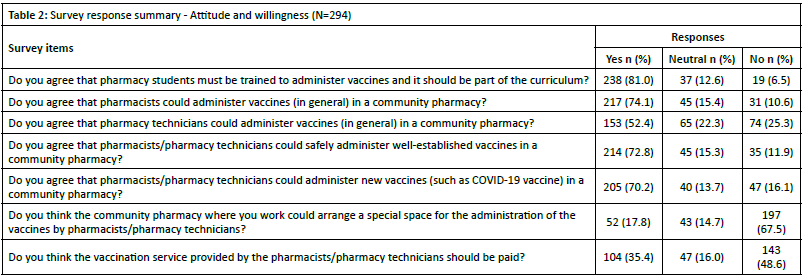
The participants’ attitudes towards administering vaccines at the community pharmacies were measured using specific survey items Table 2. The majority of the participants agreed that pharmacy students must be trained to administer vaccines and it should be part of the curriculum (81.0%), that pharmacists could administer vaccines (in general) in a community pharmacy (74.1%), that pharmacy technicians could administer vaccines (in general) in a community pharmacy (52.4%), that pharmacists/pharmacy technicians could safely administer well-established vaccines in a community pharmacy (72.8%), and that pharmacists/pharmacy technicians could administer new vaccines (as COVID-19 vaccine) in a community pharmacy (70.2%). On the other hand, most of the participants (82.2%) doubt the ability of the community pharmacy where they work to arrange a special space for the administration of the vaccines by pharmacists/pharmacy technicians.
Training needs and preferences
The training needs and training preferences of the participants were summarized in Table 3. While just about half knew how to administer vaccines (49.3%), the majority of the participants indicated their zeal to learn how to administer the intramuscular vaccine (86.4%) including those who already knew how to administer the vaccine. Moreover, about 9 in 10 participants (90.5%) also expressed their interest in learning how to administer subcutaneous vaccines. The most preferred form of training was hands-on (47.3%). They also preferred that the training has to be certified by an accredited organization (48.0%). The most preferred items for the training contents include counseling the patient (64.6%), ensuring the vaccine is
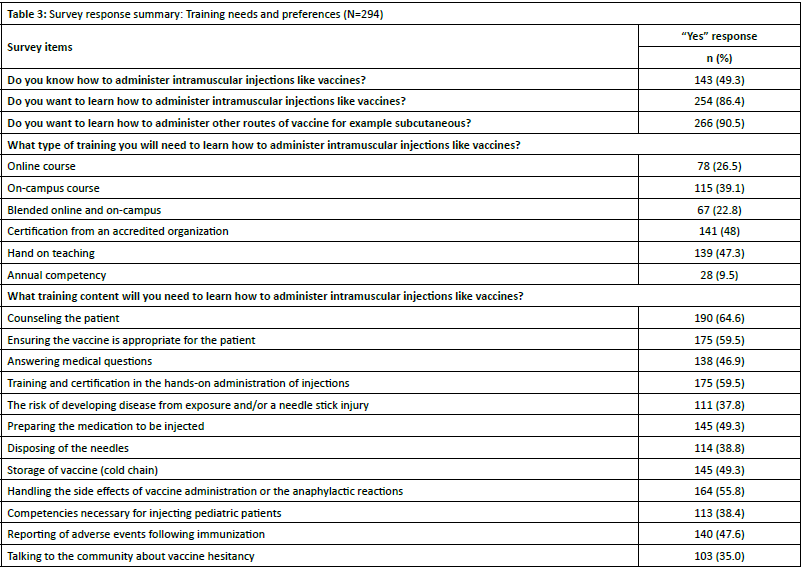
appropriate for the patient (59.5%), training and certification on the hands-on administration of injections (59.5%), and handling the side effects of vaccine administration or the anaphylactic reactions (55.8%).
Factors associated with willingness to administer vaccines
Factors associated with the willingness of the respondents to administer vaccines in the community pharmacies were explored and presented in Table 4. Having experience in administering subcutaneous during their study (AOR=4.12, 95% CI=1.06-16.81, P=0.045), as well as having the belief that pharmacy students should be trained working in a chain pharmacy (AOR=18.88, 95% CI=9.00-39.58, P<0.001) were found to significantly associated with willingness to administer vaccines in the community pharmacies after adjusting for possible confounders. All other factors explored were not found to be significantly associated with willingness Table 4.
Barriers to administering vaccines at community pharmacies
Participants also reported possible barriers to administering intramuscular vaccines in a community pharmacy (Figure 1). The most commonly reported barriers were lack of privacy (52.3%), lack of space (46.9%), and lack of skill to administer the vaccine (40.1%). On the other hand, lack of time for documentation (12.1%), cost and reimbursement (13.9%), and cultural barriers were the least reported.
DISCUSSION
The study presents an extensive insight into the attitudes, needs, and challenges that are faced by pharmacists in Abu Dhabi Emirates in regard to administering flu & COVID-19 vaccines. The study concentrates on a wide variety of factors that impact the willingness of pharmacists to take part in vaccination assistance and helps identify possible drawbacks that need to be addressed for successful implementation.
The majority of the pharmacists displayed a positive attitude towards the assistance of distributing vaccines, with significant support for incorporating vaccination training program into the pharmacy curriculum. This aligns with worldwide patterns as pharmacists are more acknowledged for their ability to improve vaccine rates thanks to their availability and credibility in local areas1. The solid enthusiasm among pharmacists to learn and administer intramuscular and subcutaneous vaccines shows the level of interest and preparation to lengthen their professional roles. A scoping review discussed that pharmacists play a crucial role in addressing worries about vaccine side effects, hesitancy and increasing vaccination rates10. They serve as advocates, educators, and providers of health promotion11,12. Moreover, a study conducted in Italy emphasized the role of the community pharmacist in counseling and addressing vaccine hesitancy among the community as they are first point of contact with the public13.
In spite of having positive feedback, the study shows a lack of certified and accredited training programs, the pharmacists’ desire for hands-on training programs that are both certified and accredited demonstrates their dedication to excellence when administering vaccines. When compared with previous research, it is consistent, showing the importance of training to prepare pharmacists with the necessary skills to safely and effectively administer vaccines9.
The absence of rooms to ensure privacy when administrating vaccines with community pharmacies is a notable barrier, with 82.2% of respondents who have stated their concerns about having a designated space for administering vaccines. This establishment is highly significant because it impacts the feasibility of offering vaccines in these kinds of environments. Challenges included inexperience and lack of knowledge of administering vaccines, along with other issues regarding managing possible adverse effects and anaphylactic reactions. These results align with worldwide issues that require
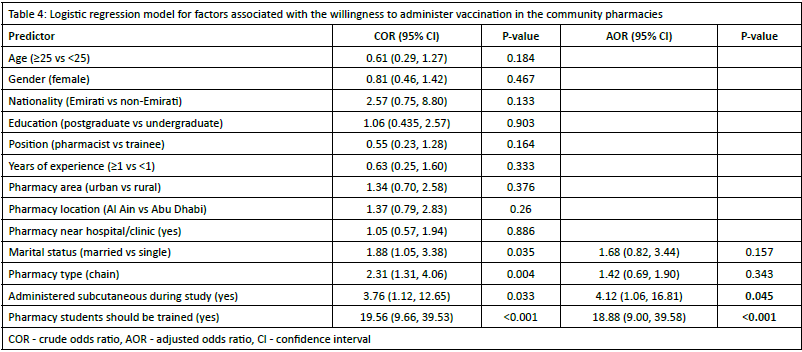
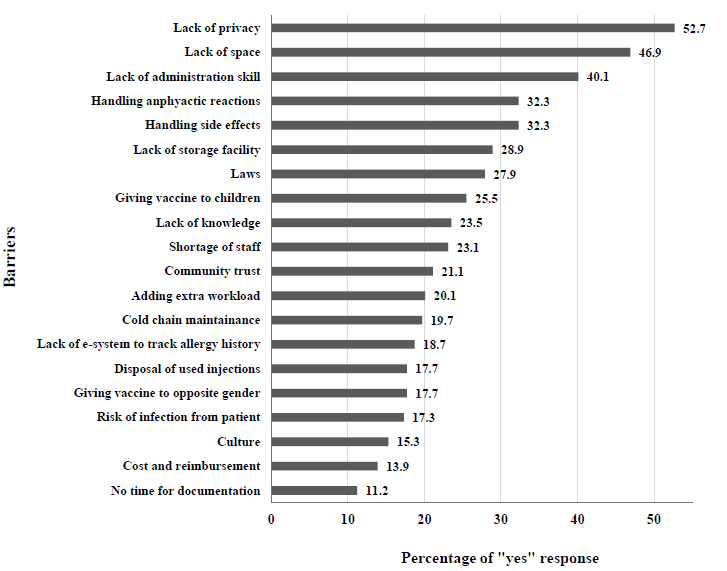
Figure 1. Barriers to administering intramuscular vaccines in a community pharmacy (N=294)
pharmacists to improve their physical infrastructure and clinical skills in order to effectively contribute to vaccination programs2. Despite the fact that giving vaccine to opposite gender and impact of culture were at the bottom of the list of barriers in our cohort, we anticipate that these barriers will get centre stage after full implementation of this service. Taking in the account the coherent culture of the UAE, cultural factors affecting vaccine administration (e.g., gender dynamics, preferences for vaccine sites) will rise to the surface. A study conducted in Jordan found that male gender was significantly correlated with increased barriers to provide the vaccine14. A literature review about cultural sensitivity and global pharmacy engagement in the Arab World study highlighted the crucial need for sensitivity toward the cultural and clinical needs of the community15,16. Moreover, the UAE community is a multiethnic community therefor there is a need for policymakers to advocate for culturally sensitive pharmacy education.
In order to integrate vaccination services in community pharmacies successfully, Policy frameworks must comprehensively cover the structural, legal, and training requirements. A consistent approach is needed to legalize and define the role of pharmacists in administering vaccines, given the varying regulatory systems across several Emirates. Additionally, establishment of guidelines that focus on subjects such as the storage of vaccines, educating patients, documenting information, and emergency response procedures will be necessary to guarantee the safe and efficient delivery of vaccines.
The study represents valuable information to stakeholders, including the Department of Health in Abu Dhabi, to help them create evidence-based plans for expanding pharmacists’ involvement in vaccination services. Overcoming the obstacles by improving infrastructure offering training programs and implementing policies is crucial, for the effective rollout of this project. Harnessing the enthusiasm and dedication of pharmacist stakeholders can improve access, to vaccines. Increase coverage, which will in turn support health objectives.
The limitations of this study span over the non-generalizability of these findings to the seven Emirates in the UAE since it was
conducted in Abu-Dhabi Emirate only. Moreover, pharmacists were selected by the Department of Health in Abu Dhabi for the piloting of this initiative and that may impact their attitude. Furthermore, a qualitative interview was not executed because pharmacists were busy and therefore, we recommend conducting focus group discussions with pharmacists to have an in-depth understanding of their attitudes and barriers. Moreover, we recommend surveying the community to see their attitudes toward the uptake of this initiative.
CONCLUSION
Community pharmacists in Abu Dhabi have a positive attitude toward administering vaccines and receiving significant support in training and education. However, obstacles need to be addressed in order for implementation to be successful. The findings from the study may be utilized to develop strategies and guidelines to help pharmacists expand their participation, leading to better health results for the public in the UAE.
References
- Yemeke TT, McMillan S, Marciniak MW, Ozawa S. A systematic review of the role of pharmacists in vaccination services in lowand middle-income countries. Research in Social and Administrative Pharmacy. 2021;17(2):300-6.
- Jennings S-L, Kucherepa U, Voyer K, Cha R. Barriers and strategies in developing an integrated immunization stewardship program in the health-system setting: The role of the pharmacist. American Journal of Health-System Pharmacy. 2021;78(24):2265-70.
- Tawfiq AM, Alomar MJ, Hassan N, Palaian S. Nationwide survey on attitudes and perceived barriers toward provision of pharmaceutical care among final year undergraduate pharmacy students in the United Arab Emirates. PloS one. 2021;16(2):e0246934.
- Rayes IK, Hassali MA, Abduelkarem AR. The role of pharmacists in developing countries: the current scenario in the United Arab Emirates. Saudi Pharmaceutical Journal. 2015;23(5):470-4.
- Basak SC, Sathyanarayana D. Pharmacy education in India. American journal of pharmaceutical education. 2010;74(4):68.
- Bhagavathula AS, Sarkar BR, Patel I. Clinical pharmacy practice in developing countries: focus on India and Pakistan. Archives of Pharmacy Practice. 2014;5(2-2014):91-4.
- Gad MZ, editor Making Pharmacy Education in Egypt Fit for the Future. Final wrap up meeting for the Tempus project JEP;
- Rahma AT, Ahmed LA, Elsheik M, Elbarazi I, Ali BR, Patrinos GP, et al. Mapping the Educational Environment of Genomics and Pharmacogenomics in the United Arab Emirates: A Mixed-Methods Triangulated Design. OMICS: A Journal of Integrative Biology. 2021;25(5):285-93.
- Turcu-Stiolica A, Kamusheva M, Bogdan M, Tadic I, Harasani K, Subtirelu M-S, et al. Pharmacist’s perspectives on administering a COVID-19 vaccine in community pharmacies in four balkan countries. Frontiers in Public Health. 2021;9:766146.
- Cassidy C, Langley J, Steenbeek A, Taylor B, Kennie-Kaulbach N, Grantmyre H, et al. A behavioral analysis of nurses’ and pharmacists’ role in addressing vaccine hesitancy: scoping review. Human Vaccines & Immunotherapeutics. 2021;17(11):4487-
- Omecene NE, Patterson JA, Bucheit JD, Andersot AN, Rogers D, Goode JV, et al. Implementation of pharmacist-administered pediatric vaccines in the United States: major barriers and potential solutions for the outpatient setting. Pharmacy Practice (Granada). 2019;17(2).
- Aldajani FN, Aldosari M. Pharmacist-led vaccination services in the Middle East. Journal of Pharmaceutical Policy and Practice. 2023;16(1):171.
- Ciliberti R, Bragazzi NL, Bonsignore A. The implementation of the professional role of the community pharmacist in the immunization practices in Italy to counteract vaccine hesitancy. Pharmacy. 2020;8(3):155.
- Jarab AS, Al-Qerem W, Mukattash TL. Community pharmacists’ willingness and barriers to provide vaccination during COVID-19 pandemic in Jordan. Human Vaccines & Immunotherapeutics. 2022;18(1):2016009.
- Alsharif NZ, Khanfar NM, Brennan LF, Chahine EB, Al-Ghananeem AM, Retallick J, et al. Cultural sensitivity and global pharmacy engagement in the Arab world. American journal of pharmaceutical education. 2019;83(4):7228.
- Mukhalalati B, Shahrour Ma, Rabie S, Awaisu A, Elshami S, Alali F. Cultural awareness and competence of pharmacy educators and learners from the perspective of pharmacy students at Qatar University: A mixed-methods approach. PloS one. 2020;15(12):e0243095.