
Epidemiology and associated factors for hospitalization-related respiratory syncytial virus infection among children less than five years of age in Saudi Arabia. A Real-World Retrospective Analysis
Hind M. ALOSAIMI. Department of Pharmacy Services Administration, King Fahad Medical City, Riyadh, Saudi Arabia.
Ghusun M. ALHAZIMI. Department of Bacteriology lab, Northern Border Regional Laboratory, Northern borders cluster, Arar, Kingdom of Saudi Arabia.
Maymunah A. ALJASIR. Department of Clinical Pharmacy, Northern Border University, Rafha, Kingdom of Saudi Arabia.
Abdulsalam A. ALHARBI. Department of Pharmacy, King Salman Specialist Hospital, Hail, Saudi Arabia.
Noura A. ALATWI. Pediatric Department, at East Jeddah General Hospital, Kingdom of Saudi Arabia.
Areej A. ALENZI. Department of Infection Control and Public Health, Regional Laboratory in Northern Border Region, Arar, Kingdom of Saudi Arabia.
Abdullah M. ALRESHEEDI. Department of Medicine, Qassim University, Kingdom of Saudi Arabia
Layla abadalwahab. Nursing department, maternity and children Hospital Dammam, Kingdom of Saudi Arabia, Dammam
Afnan saleh. Nursing department, maternity and children Hospital Dammam, Kingdom of Saudi Arabia, Dammam
Zahra Alsalem. Nursing department, maternity and children Hospital Dammam, Kingdom of Saudi Arabia, Dammam
Zahra Aljaroudi. Laboratory department, Comprehensive screening center, Kingdom of Saudi Arabia, Dammam
Ruba Alsulami. Department of medicine, University of Jeddah, Jeddah, Kingdom of Saudi Arabia.
Noof K. Alamer. Department of medicine, king Faisal University, kingdom of Saudi Arabia, Alahsa.
Atheer Alruwaili. Pharmaceutical Services Department , Northern Area Armed Forces Hospital, King Khalid Military, Hafr Al Batin 31991 , Kingdom of Saudi Arabia
Mohammed KANAN*. Department of Pharmaceutical Care, Northern Borders Cluster, Rafha Centeral Hospital, Rafha, Kingdom of Saudi Arabia. ii_kanan101@outlook.com
DOI: 10.18549/PharmPract.2025.1.3112
Abstract
Background: The rapid development, approval, and distribution of these vaccines highlight the need to carefully assess their safety. One significant concern is the incidence of Adverse Events Following Immunization (AEFI). There are few reports on the factors influencing AEFI and differences in AEFI among different COVID-19 vaccine brands in Thailand. Exploration of the incidence and factors related to post-vaccination adverse reactions against SARSCoV-2 in the population attending vaccination centers in Thailand is considered pivotal. Objective: To investigate the incidence and factors associated with adverse events following the administration of the COVID-19 vaccine in the Ubon Ratchathani province. Methods: We analyzed data from individuals who received COVID-19 vaccinations in Ubon Ratchathani province between June 1, 2021, and July 31, 2022. Results: The study examined data from 2,955,978 COVID-19 vaccines administered in Ubon Ratchathani province. Among these, 3.34% experienced an AEFI, further categorized into events occurring within 30 min (0.17%) and after 30 min (3.19%) of vaccination. The occurrences were higher in females compared to males. The age groups exhibited distinct AEFI rates, with children aged 5–17 years and adults aged 18–60 years facing a higher risk. Additionally, individuals with comorbidities are more likely to experience AEFI. The brand of the vaccine and the number of doses administered also influenced AEFI rates. This comprehensive analysis provides valuable insights into AEFI reports, vaccine brands, and associated risk factors, and offers crucial information for vaccine safety monitoring and management. Conclusion: This COVID-19 vaccine adverse events study revealed that higher odds of adverse events were associated with being female, younger, having comorbidities, brand of vaccines, or getting over two doses. These findings provide valuable real-world safety information regarding different COVID-19 vaccines, aiding healthcare professionals and policymakers in effectively monitoring and managing vaccine-related AEFI.
Keywords: factors; adverse events following immunization (AEFI); covid-19 vaccine; Thailand
INTRODUCTION
Respiratory Syncytial Virus (RSV) infection is a significant cause of respiratory illness among children worldwide, particularly in those under the age of 5.1 Respiratory viruses are common worldwide, and environmental, demographic, socioeconomic, and geographic factors influence their frequency and transmission.2 Acute respiratory tract infections (ARTIs) are a leading global cause of pediatric morbidity and mortality. 3 ARTIs are caused mainly by viruses, with lesser amounts of bacteria and fungus contributing as well.4 Between 40-90% of ARTIs in underdeveloped nations are caused by viral infections. 5 (RSV) and influenza virus (flu) are expected to cause 58,000 and 76,000 fatalities annually, respectively. 6 Respiratory infections affect both adults and children, and they are reflected in a large number of hospital and emergency room visits (e.g., in the United States, there are 140,000 to 710,000 flu-related hospitalizations per year), where respiratory viral infection is the most common reason to seek medical care.8
In Saudi Arabia, RSV poses a substantial burden on pediatric healthcare services, leading to a considerable number of hospitalizations and associated healthcare costs.8 Between 2001 and 2015, RSV infection was responsible for over 23% of acute respiratory diseases in the pediatric population in Saudi Arabia; the majority of these cases involved children under the age of one year.9 The polymerase chain reaction test determined that RSV infection caused 53% and 64% of general ward admissions and pediatric intensive care unit (PICU) admissions, respectively, for children aged < 6 years (median five months) hospitalized with bronchiolitis in Saudi Arabia.10
Despite advancements in medical science and healthcare infrastructure, RSV remains a formidable challenge due to its high transmissibility and propensity to cause severe respiratory illness, including bronchiolitis and pneumonia, especially in vulnerable pediatric populations.11 The burden of RSVassociated hospitalizations extends beyond immediate health impacts, often leading to long-term respiratory complications and economic strain on families and healthcare systems.12
Given Saudi Arabia’s diverse geographical and climatic conditions, variations in RSV epidemiology and associated risk factors may exist across different regions of the country.13 Factors such as crowded living conditions, air pollution, and inadequate access to healthcare services in certain areas may exacerbate the risk of RSV transmission and the severity of illness among children under five years old.14
This research article aims to provide a comprehensive analysis of the epidemiology of RSV-related hospitalizations among children less than five years of age in Saudi Arabia. By identifying the associated risk factors, including age, gender, preterm birth, underlying medical conditions, and environmental factors, this study seeks to contribute valuable insights into preventing and managing RSV infections in the pediatric population. Understanding the epidemiological trends and risk factors specific to Saudi Arabia can inform targeted public health interventions, vaccination strategies, and clinical management protocols to mitigate the impact of RSV on children’s health and well-being in the region.
METHODOLOGY
Study design and population
A retrospective study was conducted at King Fahad Medical City in Riyadh, Kingdom of Saudi Arabia (KSA), based on secondary data analysis of the electronic medical record. The data was collected during the period from January 2019 to December 2023. The inclusion criteria for the study were Age up to 5 years, diagnosis of respiratory infection, and a positive result for a nasopharyngeal swab of RSV in testing using either an RT-PCR assay or fast antigen testing. All patients’ clinical data and laboratory test results were gathered. Clinical variables such as patient characteristics, clinical signs and symptoms, medical diagnosis, length of hospital stay, and blood sample laboratory test were also collected. We chose patients whose diagnoses were based on the 10th version of the International Classification of Diseases.15
ETHICAL APPROVAL
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board Institutional Review Board of King Fahad Medical City, Riyadh, KSA under IRB log Number: 23-525.
Data collection
The review of electronic and paper medical charts collected baseline data on each patient, including underlying diseases, length of hospital stay, and diagnosis type (primary diagnosis of RSV infection, co-morbidity with an underlying disease, and complication from another diagnosis). A history of fever, cough, sputum production, dyspnea, rhinorrhea, sneezing, wheezing, sore throat, nausea, cyanosis, pallor, diarrhea, chest discomfort, convulsions, decreased breath sound, and needing mechanical ventilation was among the symptoms and indicators. The pre-term newborn reference was less than 38 weeks gestation.16 The following conditions were included in collecting underlying diseases: hematological conditions, neurological disorders, gastrointestinal disorders, kidney disorders, and cardiac and pulmonary ailments. Primary or secondary discharge diagnoses could be the underlying medical issues.17 Furthermore, laboratory analysis blood tests, including those for hemoglobin (Hb), white blood cells (WBC), platelets, neutrophils, eosinophils, monocytes, and lymphocytes, were obtained using an electronics laboratory record on the day of hospital admission or the initial visit.
Data analysis
We first tallied the total number of RSV cases for descriptive data analysis. We separated them into two groups based on the patient admission types: the outpatient department (OPD) and the in-patient department (IPD). We performed univariable and multivariable binomial regression analysis to evaluate RSV-related hospitalizations in young children. The final model, which included variables significant at the 5% significance level, was chosen using the best subset approach. Calculations were made for crude and corrected odd ratios and 95% confidence intervals. P-values less than 0.05 were regarded as statistically significant. In multivariable logistic regression models (adjusted odds ratio: aOR), variables that showed significant relationships with RSV-related hospitalizations and infections in univariable logistic regression models (crude odds ratio: cOR) were retained. For the data analysis, we used SPSS (version 27).
RESULTS
Prevalence of RSV
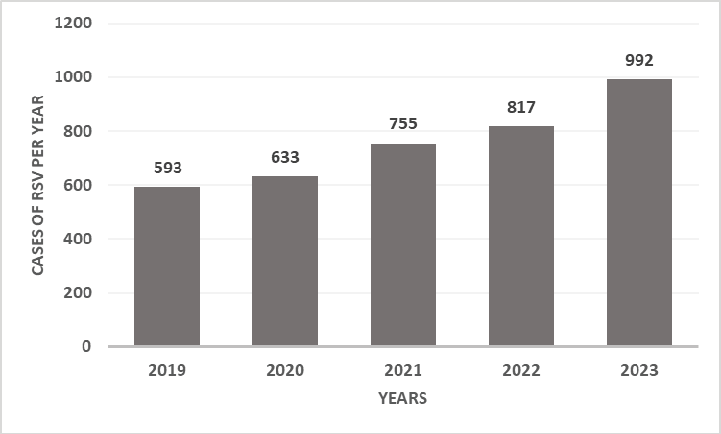
In five years, 3790 patients were admitted. Subsequently, 593, 633, 755, 817, and 992 patients were admitted from 2019 to 2023. These results can be visualized in Figure 1.
Clinical Characteristics of RSV
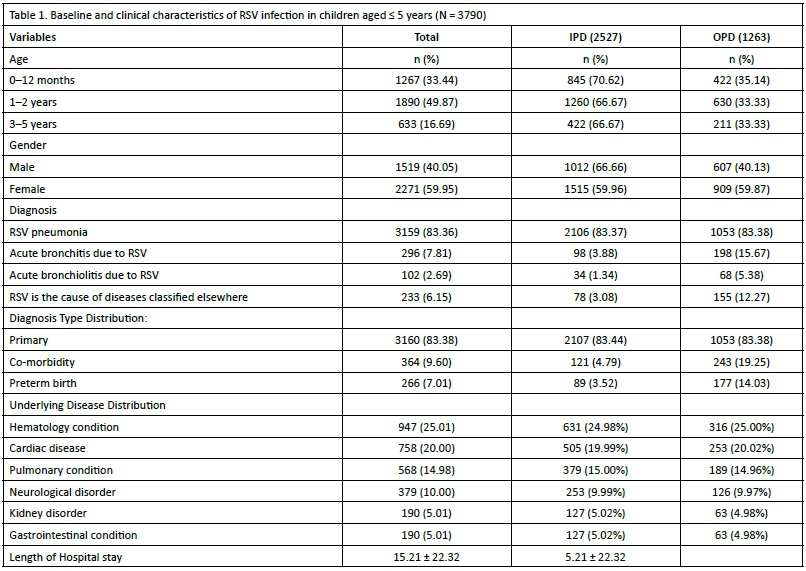
The majority of patients were in the age groups of 1-2 years (49.87%) and 0-12 months (33.44%), with fewer patients aged 3-5 years (16.69%). There were slightly more female patients (59.95%) than male patients (40.05%). RSV pneumonia was the most common diagnosis (83.36%), followed by acute bronchitis due to RSV (7.81%) and acute bronchiolitis due to RSV (2.69%). The average length of hospital stay was 15.21 days, with a standard deviation of 22.32 days, indicating considerable variability in the duration of hospitalization. The results are presented in Table 2.
Symptoms associated with RSV
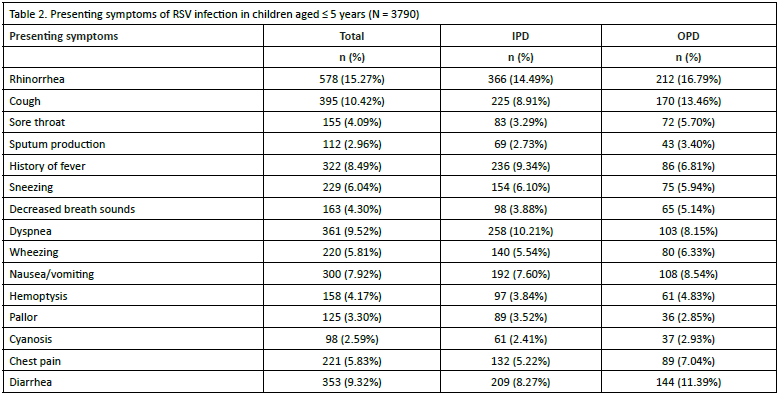
A runny nose was the most common symptom reported, with 15.27% of patients experiencing it. Among hospitalized patients (IPD), the percentage was slightly lower at 14.49%, while in outpatient department (OPD) patients, it was marginally higher at 16.79%. Cough was reported by 10.42% of patients, with a similar distribution between IPD (8.91%) and OPD (13.46%). The sore throat was reported by 4.09% of patients, with a slightly higher prevalence in OPD (5.70%) than in IPD (3.29%). Tables should be placed in the main text near the first time they are cited. These results are tabulated in Table 2.
Laboratory blood test analysis
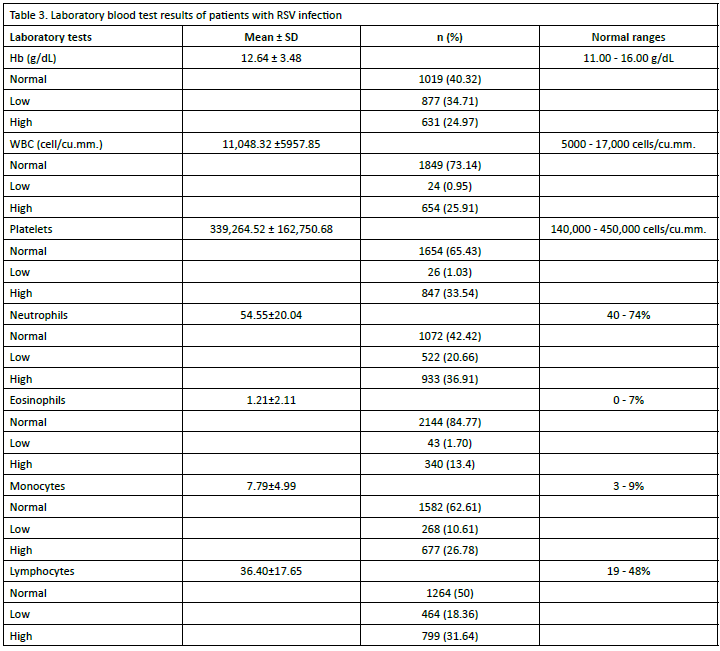
The mean Hb level was 12.64 ± 3.48 g/dL. The majority (40.32%) had normal Hb levels, while 34.71% had low levels and 24.97% had high levels. Normal range: 11.00 - 16.00 g/dL. The mean WBC count was 11,048.32 ± 5957.85 cells/cu.mm. Most patients (73.14%) had average WBC counts, while 0.95% had low counts, and 25.91% had high counts. Typical range: 5000 - 17,000 cells/cu.mm. The mean platelet count was 339,264.52 ± 162,750.68 cells/cu.mm. The majority (65.43%) had average platelet counts, while 1.03% had low counts and 33.54% had high counts. Typical range: 140,000 - 450,000 cells/cu.mm. The mean neutrophil percentage was 54.55 ± 20.04%. The results are explained in Table 3.
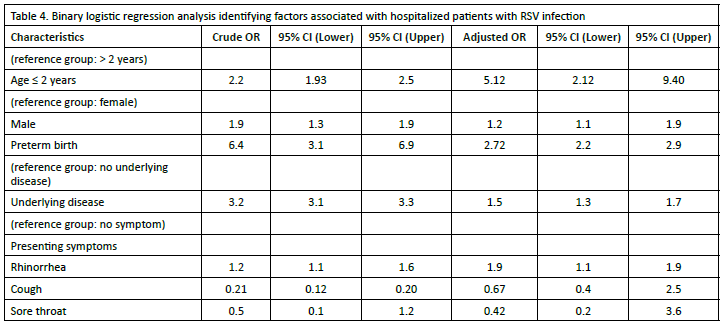
Factors associated with hospitalized pediatric patients with RSV infection
Children aged two years or younger had a significantly higher odds ratio (OR) of 2.2 (95% CI: 1.93 - 2.5) for the outcome compared to those older than two years. This association remained significant after adjusting for other factors, with an adjusted OR of 5.12 (95% CI: 2.12 - 9.40). Males had a crude OR of 1.9 (95% CI: 1.3 - 1.9) for the outcome compared to females. After adjustment, the association was slightly attenuated but still significant, with an adjusted OR of 1.2 (95% CI: 1.1 - 1.9). Preterm birth was strongly associated with the outcome, with a crude OR 6.4 (95% CI: 3.1 - 6.9). After adjustment, this association remained significant, with an adjusted OR of 2.72 (95% CI: 2.2 - 2.9). The presence of underlying disease showed a crude OR of 3.2 (95% CI: 3.1 - 3.3) for the outcome. However, after adjustment, the association was attenuated but still significant, with an adjusted OR of 1.5 (95% CI: 1.3 - 1.7). The results are explained in Table 4.
DISCUSSION
Based on a review of medical records, this study provided evidence that RSV is a dangerous virus in young children. Hospitalized children with RSV infection were frequently linked to baseline features, underlying illnesses, and presenting symptoms, according to our retrospective investigation. More than half of the hospitalized children were younger than two years old, making up most of the young patients. Previous research from Saudi Arabia and other countries showed more significant proportions of infection in children under one-yearold and also found similar infection rates.13,18 The younger
age groups are more susceptible to infections, possibly as a result of increased pathogen exposure, weakened maternal antibodies that prevent viral infections after six months of life, low viral clearance from immature immunity, and unsanitary living conditions.9,19
In this study, pulmonary and cardiovascular diseases were prevalently present, with young children or newborns making up the majority of the patient population. The majority of hospitalized RSV patients experienced several symptoms. Usually, these symptoms don’t appear all at once; they come on gradually. RSV-associated LRTI is still very common in infants, especially in those under the age of one year.20 Comorbidities of prematurity, low birth weight, cardiac disease, gastrointestinal problems, and neurological disorders were other correlation findings for risk variables in the prior study.21
In young children, gender was a factor linked to RSV infection (Table 4). According to our research, the male gender was protective against hospital-related RSV infection in children, with an odds ratio of 1.2 (95% confidence interval [CI] = 1.1–1.9). In contrast to earlier research, this study produced different findings.22,23 From the evidence base, a boy infected with RSV in infancy was associated with developing asthma in adolescence.24 It’s plausible that despite having identical exposure to respiratory pathogens, boys were more likely to acquire infections severe enough to require hospitalization because they had a higher frequency of underlying asthma. However, there could be other reasons at play.25 Therefore, keeping a close eye on male patients’ RSV infection is important.
Pneumonia was communal in our study and was similar to the previous studies.29 In hospitalized patients, pneumonia caused by RSV was present in 83.36% of children (Table 1). The clinical signs and symptoms of pneumonia are fever, difficulty breathing, dyspnea, and wheezing in general. In our study, we might assume the frequency of the presenting symptoms related to pneumonia with RSV. Similar findings were made by Turner and colleagues (2012), who discovered that patients who presented at a younger age had a significantly higher likelihood of having RSV detected (OR = 21.2, 95% CI = 5.1–88.2, p < 0.001).30 They also discovered that RSV-associated pneumonia was more severe in the youngest age group (less than five years).
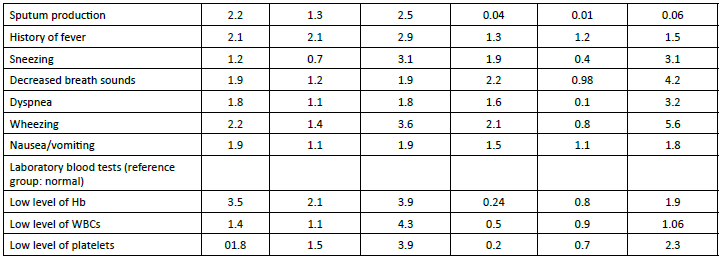
Infants experienced reduced lung development, insufficient immunity, or a higher risk of catching a respiratory disease from a household member.31 This study’s results showed that low Hb levels were associated with RSV-related hospitalization in children (cOR = 3.5, 95 % CI = 2.1–3.9. Our results support that RSV infection is associated with decreased Hb in children. Our findings support the theory that childhood RSV infection is linked to reduced Hb. Therefore, we believe this virus—at least the ones frequently found in our hospital—has something to do with how RSV affects hemoglobin. A comparison investigation between Taiwanese infants (less than five years old) infected with RSV and those without bacterial co-infection was carried out in 2022 by Lin et al.32 Reduced hemoglobin levels (aOR = 1.36; 95% CI = 1.01–1.89, p = 0.042) were associated with an increased risk of hospitalization for red-blood cell illness.33 RSV’s specific mechanism of action on Hb is unknown.34
It is abundantly evident from the data that several variables are linked to RSV infection and negatively impact newborns. Although they are constantly being researched, vaccines are the most effective means of preventing respiratory diseases. On the other hand, a single dosage of monoclonal antibodies (mAbs) in high-risk populations may be sufficient to prevent RSV infections throughout the RSV season.35 Children in Saudi Arabia who are susceptible to RSV infection have not been given mAbs. Treatments have only been given to RSV-infected children depending on their clinical presentations. Therefore, taking precautions based on transmission is the most effective strategy to stop the spread of infection through contact and drop-let pathways. To enhance treatment outcomes, specific treatments for RSV-associated LRTI need to be investigated, and children who have a history of low Hb levels should exercise particular caution. To lessen the burden of the illness, the public health system should also suggest looking into laboratory blood tests for kids with respiratory infections.
There were various restrictions on this investigation. First of all, it happened in a single site and might not apply to other regions. Furthermore, since this was a retrospective study, some data might have been missing. Third, the study’s data were taken from ICD-10 codes, which are prone to error.
CONCLUSIONS
RSV is a major reason for young children’s hospital admissions. Our results showed that the primary factors linked to RSVrelated hospitalizations were underlying illness and presenting symptoms, particularly sputum production preterm birth in young children under the age of five years. Furthermore, a major contributing factor to children being hospitalized with RSV infection was their low hemoglobin level and pneumonia. The significance of increasing public awareness of the cause of RSV infection in this community has to be highlighted in light of these facts.
AUTHOR CONTRIBUTIONS:
Conceptualization: HMA. GMA MKA and AAA; methodology: NAA, ASA, RHA; software: AAA, SPA, SAD; validation: NMA, ENA, FSA, AMA; formal analysis: HOA MAK; investigation: GMA, AAA, MAA, ASA; resources, MAK; data curation: RHA, SPA, ENA, NMA; writing-original draft preparation: HMO, FSA, AMA, RHA, MAK; writing-review and editing: HMO. SAD, NMA, ENA; visualization: MAK, HOM; supervision: HOM, MAK; project administration: MAK, HOM; funding acquisition: MAK. All authors have read and agreed to the published version of the manuscript.
ACKNOWLEDGMENT:
The authors would like to thank the Research Center at King Fahd Medical City, Riyadh Second Health Cluster, for their valuable technical support provided for the manuscript
CONFLICTS OF INTEREST:
The authors declare no conflicts of interest.
FUNDING:
This research received no external funding.
References
1. Li Y, Wang X, Blau DM, Caballero MT, Feikin DR, Gill CJ, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. The Lancet. 2022;399(10340):2047-64. https://doi.org/10.1016/s0140-6736(22)00478-0
2. Ahmed A, Alsenaidy AM, Mobaireek KF, AlSaadi MM. Viral etiology of acute respiratory infections during 2014–2016 in Riyadh, Saudi Arabia. Future Virology. 2022;17(5):269-80.
3. Dhamotharan J, Kumar DPD, Rajasekaran LRS, Mondal V, Selvan RP, Shaik SAM, et al. Assessing the Quality of Life of Children’s with Acute Respiratory Tract Infections. Indian Journal of Pharmacy Practice. 2021;14(1).
4. Khasawneh AI, Himsawi NM, Abu-Raideh JA, Sammour A, Abu Safieh H, Obeidat A, et al. Prevalence of SARS-COV-2 and other respiratory pathogens among a Jordanian subpopulation during Delta-to-Omicron transition: Winter 2021/2022. PLoS One. 2023;18(3):e0283804. https://doi.org/10.1371/journal.pone.0283804
5. Suryadevara M, Domachowske JB. Epidemiology and seasonality of childhood respiratory syncytial virus infections in the tropics. Viruses. 2021;13(4):696. https://doi.org/10.3390/v13040696 6. Chorazka M, Flury D, Herzog K, Albrich WC, Vuichard-Gysin D. Clinical outcomes of adults hospitalized for laboratory-confirmed respiratory syncytial virus or influenza virus infection. Plos one. 2021;16(7):e0253161. https://doi.org/10.1371/journal. pone.0253161
7. Hanula RJ. Influenza Therapeutics: Evaluating the Benefits and Harms of Oseltamivir and Corticosteroids: McGill University (Canada); 2022.
8. Alharbi AS, Alzahrani M, Alodayani AN, Alhindi MY, Alharbi S, Alnemri A. Saudi experts’ recommendation for RSV prophylaxis in the era of COVID-19: Consensus from the Saudi Pediatric Pulmonology Association. Saudi Medical Journal. 2021;42(4):355- 362. https://doi.org/10.15537/smj.2021.42.4.20200769
9. Alharbi AS, Alqwaiee M, Al-Hindi MY, Mosalli R, Al-Shamrani A, Alharbi S, et al. Bronchiolitis in children: The Saudi initiative of bronchiolitis diagnosis, management, and prevention (SIBRO). Annals of thoracic medicine. 2018;13(3):127-43. https://doi. org/10.4103/atm.atm_137_18
10. Alharbi A, Yousef A, Zubani A, Alzahrani M, Al-Hindi M, Alharbi S, et al. Respiratory Syncytial Virus (RSV) Burden in Infants in the Kingdom of Saudi Arabia and the Impact of All-Infant RSV Protection: A Modeling Study. Advances in Therapy. 2024: 41(4):1419-35.https://doi.org/10.1007/s12325-024-02798-w
11. Stambas J, Lu C, Tripp RA. Innate and adaptive immune responses in respiratory virus infection: Implications for the clinic. Expert review of respiratory medicine. 2020;14(11):1141-7. https://doi.org/10.1080/17476348.2020.1807945
12. Young M, Smitherman L. Socioeconomic impact of RSV hospitalization. Infectious diseases and therapy. 2021;10(Suppl 1):35- 45. https://doi.org/10.1007/s40121-020-00390-7
13. Yassine HM, Sohail MU, Younes N, Nasrallah GK. Systematic review of the respiratory syncytial virus (RSV) prevalence, genotype distribution, and seasonality in children from the Middle East and North Africa (MENA) region. Microorganisms. 2020;8(5):713. https://doi.org/10.3390/microorganisms8050713
14. Na’amnih W, Kassem E, Tannous S, Kagan V, Jbali A, Hanukayev E, et al. Incidence and risk factors of hospitalisations for respiratory syncytial virus among children aged less than 2 years. Epidemiology & Infection. 2022;150:e45. https://doi.org/10.1017/s0950268822000152
15. Ramrakhiani NS, Le MH, Yeo YH, Le AK, Maeda M, Nguyen MH. Validity of international classification of diseases, tenth revision, codes for cirrhosis. Digestive diseases. 2021;39(3):243-6. https://doi.org/10.1159/000510981
16. Sharma D, Padmavathi IV, Tabatabaii SA, Farahbakhsh N. Late preterm: a new high risk group in neonatology. The Journal of Maternal-Fetal & Neonatal Medicine. 2021;34(16):2717-30. https://doi.org/10.1080/14767058.2019.1670796
17. Kim L, Garg S, O’Halloran A, Whitaker M, Pham H, Anderson EJ, et al. Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the US coronavirus disease 2019 (COVID-19)-associated hospitalization surveillance network (COVID-NET). Clinical infectious diseases. 2021;72(9):e206-e14. https://doi.org/10.1093/ cid/ciaa1012
18. Fagbo SF, Garbati MA, Hasan R, AlShahrani D, AlShehri M, AlFawaz T, et al. Acute viral respiratory infections among children in MERSendemic Riyadh, Saudi Arabia, 2012–2013. Journal of Medical Virology. 2017;89(2):195-201. https://doi.org/10.1002/ jmv.24632
19. Khamis F, AlKobaisi M, AlAreimi W, AlKindi H, AlZakwani I. Epidemiology of respiratory virus infections among infants and young children admitted to hospital in Oman. Journal of medical virology. 2012;84(8):1323-9. https://doi.org/10.1002/ jmv.23330
20. Coultas JA, Smyth R, Openshaw PJ. Respiratory syncytial virus (RSV): a scourge from infancy to old age. Thorax. 2019;74(10):986- 93. https://doi.org/10.1136/thoraxjnl-2018-212212
21. Jadcherla SR, Wang M, Vijayapal AS, Leuthner SR. Impact of prematurity and co-morbidities on feeding milestones in neonates: a retrospective study. Journal of Perinatology. 2010;30(3):201-8. https://doi.org/10.1038/jp.2009.149
22. Cedrone F, Montagna V, Del Duca L, Camplone L, Mazzocca R, Carfagnini F, et al. Epidemiology of Bronchiolitis and Respiratory Syncytial Virus and Analysis of Length of Stay from 2015 to 2022: Retrospective Observational Study of Hospital Discharge Records from an Italian Southern Province before and during the COVID-19 Pandemic. Diseases. 2024;12(1):17. https://doi. org/10.3390/diseases12010017
23. Mondì V, Paolillo P, Bedetta M, Lucangeli N, Picone S. Exploring the adoption of less restricted criteria for respiratory syncytial virus prophylaxis in late preterm infants: insights from a retrospective analysis. Frontiers in Pediatrics. 2023;11:1154518. https://doi.org/10.3389/fped.2023.1154518
24. Rubner FJ, Jackson DJ, Evans MD, Gangnon RE, Tisler CJ, Pappas TE, et al. Early life rhinovirus wheezing, allergic sensitization, and asthma risk at adolescence. Journal of Allergy and Clinical Immunology. 2017;139(2):501-7. https://doi.org/10.1016/j. jaci.2016.03.049
25. Pérez-Yarza EG, Moreno A, Lázaro P, Mejías A, Ramilo O. The association between respiratory syncytial virus infection and the development of childhood asthma: a systematic review of the literature. The Pediatric infectious disease journal. 2007;26(8):733-9. https://doi.org/10.1097/inf.0b013e3180618c42
26. Aikphaibul P, Theerawit T, Sophonphan J, Wacharachaisurapol N, Jitrungruengnij N, Puthanakit T. Risk factors of severe hospitalized respiratory syncytial virus infection in tertiary care center in Thailand. Influenza and Other Respiratory Viruses. 2021;15(1):64-71. https://doi.org/10.1111/irv.12793
27. Naorat S, Chittaganpitch M, Thamthitiwat S, Henchaichon S, Sawatwong P, Srisaengchai P, et al. Hospitalizations for acute lower respiratory tract infection due to respiratory syncytial virus in Thailand, 2008–2011. The Journal of infectious diseases. 2013;208(suppl_3):S238-S45. https://doi.org/10.1093/infdis/jit456
28. Chuaychoo B, Ngamwongwan S, Kaewnaphan B, Athipanyasilp N, Horthongkham N, Kantakamalakul W, et al. Clinical manifestations and outcomes of respiratory syncytial virus infection in adult hospitalized patients. Journal of Clinical Virology. 2019;117:103-8. https://doi.org/10.1016/j.jcv.2019.07.001
29. Bunthi C, Baggett HC, Gregory CJ, Thamthitiwat S, Yingyong T, Paveenkittiporn W, et al. Enhanced surveillance for severe pneumonia, Thailand 2010–2015. BMC Public Health. 2019;19(Suppl 3):472. https://doi.org/10.1186/s12889-019-6774-5
30. Turner C, Turner P, Cararra V, Eh Lwe N, Watthanaworawit W, Day NP, et al. A high burden of respiratory syncytial virus associated pneumonia in children less than two years of age in a South East Asian refugee population. PloS one. 2012;7(11):e50100. https://doi.org/10.1371/journal.pone.0050100
31. Jha A, Jarvis H, Fraser C, Openshaw P. Respiratory syncytial virus. SARS, MERS and other viral lung infections. 2016.
32. Lin H-C, Liu Y-C, Hsing T-Y, Chen L-L, Liu Y-C, Yen T-Y, et al. RSV pneumonia with or without bacterial co-infection among healthy children. Journal of the Formosan Medical Association. 2022;121(3):687-93. https://doi.org/10.1016/j.jfma.2021.08.012
33. Epstein D, Nasser R, Mashiach T, Azzam ZS, Berger G. Increased red cell distribution width: a novel predictor of adverse outcome in patients hospitalized due to acute exacerbation of chronic obstructive pulmonary disease. Respiratory medicine. 2018;136:1-7. https://doi.org/10.1016/j.rmed.2018.01.011
34. Griffiths C, Drews SJ, Marchant DJ. Respiratory syncytial virus: infection, detection, and new options for prevention and treatment. Clinical microbiology reviews. 2017;30(1):277-319. https://doi.org/10.1128/cmr.00010-16
35. Messina A, Germano C, Avellis V, Tavella E, Dodaro V, Massaro A, et al. New strategies for the prevention of respiratory syncytial virus (RSV). Early Human Development. 2022;174:105666. https://doi.org/10.1016/j.earlhumdev.2022.105666